source-library
TRANSGENDER ISSUES
Medical Consensus
Medical Consensus
This is an incomplete list of the reputable scientific & social organizations which affirm the validity of transgender people (that transness is not an illness, that trans people deserve access to transgender healthcare, etc). This also serves as a list of the institutions which recognize the difference between sex and gender. This list was compiled by the TLDEF and they should be cited when referring to this list.
- American Academy of Child and Adolescent Psychiatry
- American Academy of Dermatology
- American Academy of Family Physicians
- American Academy of Nursing
- American Academy of Pediatrics
- American Academy of Physician Assistants
- American College Health Association
- American College of Nurse-Midwives
- American College of Obstetricians and Gynecologists
- American College of Physicians
- American Counseling Association
- American Heart Association
- American Medical Association
- American Medical Student Association
- American Nurses Association
- American Osteopathic Association
- American Psychiatric Association
- American Psychological Association
- American Public Health Association
- American Society of Plastic Surgeons
- Endocrine Society
- GLMA: Health Professionals Advancing LGBTQ Equality
- National Association of Nurse Practitioners in Women’s Health
- National Association of Social Workers
- National Commission on Correctional Health Care
- Pediatric Endocrine Society
- Society for Adolescent Health and Medicine
- World Medical Association
- World Professional Association for Transgender Health
Medical Transition
Medical Transition
Medical transition decreases dysphoria, suicide attempts, and improves depression and anxiety. However, most research on this subject is very low quality so we should be open to conducting better future research.
- Murad et al. 10
- Meta-analysis of 28 studies on transition and hormones
- Sex reassignment/hormonal improvements:
- 80% of individuals reported significant improvement in dysphoria
- 78% of individuals reported significant improvement in psychological symptoms
- 72% of individuals reported significant improvement in sexual function
- Positive results across the board, EVEN IN 15-YEAR FOLLOWUPS
- Low quality evidence, see methodology. Broader limitations to study quality for this topic are discussed here. Still significant and helpful findings regardless.
- Meta-analysis of 28 studies on transition and hormones
- De Vries et al. 14
- Longitudinal study on the effectiveness of puberty suppression, hormones, and later sex reassignment surgery on trans individuals in improving mental outcomes
- 55 trans youth (22 transfem and 33 transmasc) were followed over an 8 year period from before starting blockers (mean aged 13.6 years)
- While many studies like this compare those after treatment to those before treatment, this study also made comparisons to the general population and still found that psychological function was on par or better.
- “After gender reassignment, in young adulthood, the GD was alleviated and psychological functioning had steadily improved. Wellbeing was similar to or better than same-age young adults from the general population.”
- Green et al. 22
- Use of GAHT was associated with lower odds of recent depression and seriously considering suicide compared to those who wanted GAHT but did not receive it.
- For youth under age 18, GAHT was associated with lower odds of recent depression and of a past-year suicide attempt.
- “Findings support a relationship between access to GAHT and lower rates of depression and suicidality among transgender and nonbinary youth.”
- The Endocrine Society 15
- “A new study has confirmed that transgender youth often have mental health problems and that their depression and anxiety improve greatly with recognition and treatment of gender dysphoria”
- Nobili 18
- Longitudinal meta-analysis which indicates transgender people have a lower quality of life than the general population.
- However, that quality of life rises dramatically with ‘Gender Affirming Treatment’, the nature of which is detailed extensively in-text.
-
https://hqlo.biomedcentral.com/articles/10.1186/s12955-020-01510-0
-
https://www.jahonline.org/article/S1054-139X(21)00568-1/fulltext
-
https://link.springer.com/article/10.1007/s11920-021-01245-9 2021 literature review
- Almazan & Keuroghlian 2021
- Study that uses data from the US Transgender Survey (massive survey of 27,000+ people) and does a covariate analysis to learn about the association between medical transition and several mental health indicators
- Accounted for various demographic indicators including wealth (a neat finding about wealth was that those with wealth also tend to have better access to gender-affirming care, and thus were more able to benefit from that care)
- Finds that “TGD people with a history of gender-affirming surgery had significantly lower odds of past-month psychological distress, past-year tobacco smoking, and past-year suicidal ideation compared with TGD people with no history of gender-affirming surgery”
- Deeper in the study they reaffirm that its conclusions support gender-affirmative care, in line with past smaller-scale studies. “The association observed between gender-affirming surgeries and reduction in substance use behaviors is consistent with previous studies involving small community samples that demonstrated associations between gender-affirming medical care and lower odds of high-risk substance use.” and “This investigation offers evidence to support the clinical practice of gender-affirming surgery.”
- Some clear limitations e.g. association doesn’t necessarily mean causation. This study is included in the list mainly due to the large sample it’s able to pull from. Use it with this in mind.
- DO NOTE CITE THIS SOURCE: Cornell University, “What does the scholarly research say about the effect of gender transition on transgender well-being?”
- Commonly cited source in favor of gender transition, however it’s flawed and those flaws have been known about for a while now.
- The study suffers from poor categorization among other things. For example, a study with some positive and some negative results could be judged by Cornell as fitting in the “positive results” category, misrepresenting the overall pool of evidence on a subject with more nuance.
- Many of the studies suffer from small sample sizes, weak methodology, and sampling that can’t be generalized to transitioners more broadly (though some of this is to be expected from the field in general, see next point).
- The majority of studies on the subject involve very small sample sizes which somewhat undermines their reliability. This is to be expected for the field though, due to the small size of the trans population (small populations are harder to get large samples of), so that’s ultimately to be expected.
Long-term Follow-ups:
- Weyers et al. 09
- 50 MtF trans people who had done SRS 6 months earlier
- In long-term follow-ups, trans women “function well on a physical, emotional, psychological and social level”
- However, they have problems when it comes to arousal, lubrication, and pain - a minor trade-off for the previously mentioned well-being measures
- Ruppin & Pfäfflin 15
- 71 trans people (35 MtF and 36 FtM) in follow-ups ranging from 10-24 years (mean: 13.8 years)
- Trans people reported being just fine in long-term follow-up, as well as having reduced gender dysphoria
- Johansson et al. 10
- 60 trans people in Sweden in 5 year follow-ups
- No one regretted SRS or being trans
- https://link.springer.com/article/10.1007/s10508-014-0300-8
- Might be 50 years but need to check
- “A total of 15 individuals (5 FM and 10 MF) out of 681 who received a new legal gender between 1960 and 2010 applied for reversal to the original sex (regret applications). This corresponds to a regret rate of 2.2 % for both sexes (2.0 % FM and 2.3 % MF)”
-
https://pubmed.ncbi.nlm.nih.gov/9031580/ follow-up for each participant happened ‘no less than 1 year’ after surgery
- https://www.inverse.com/article/59830-gender-incongruence-transgender-surgey-survey
Important note on study quality (applicable to some other sections too):
For some research topics like medical transition, it’s very hard to get gold-standard study designs for a number of practical and ethical reasons. I’ll be pulling relevant info from this blog post which largely focuses on a different topic yet has some good info for this. In this segment it talks about how having blinded studies and control groups (two ways to improve a study’s quality) is next to impossible for researchers to do here:
- “One problem with medical treatment (and obviously surgery) for transsexuals is that blinding of studies is not possible. It is immediately obvious whether a participant received treatment or not, substitution by placebo will not work for obvious reasons. Clearly, all sex reassignment studies thus fail the gold standard.”
- “The next issue is including a [transgender] control group into the study. This would require to properly diagnose transsexuals, making sure they meet the requirements and indications for sex reassignment surgery, and then to randomly split the participants into two groups – one receiving surgery and one not… In reality, you would find the pressure transsexuals find themselves under grow so much that a large part of the untreated group commits suicide (Haas, Rodgers, Herman 2014) or seeks treatment illegally or abroad. This makes such a study highly unethical, it would never get the okay from an approvals body!”
So that leaves us with a much more limited set of options for how we can measure the outcomes of medical transition. These measures, while typically giving us lower quality results, are at least possible to conduct and studies have indeed been conducted with them. The blog lists a few of these options:
- measure the quality of life of participants before and after sex reassignment surgery (longitudinal study)
- measure the quality of life of participants after surgery and compare them to the average quality of life of transsexuals before surgery (demographics etc. need to be similar)
- simply ask transsexuals after surgery whether they feel better (yes, it is that easy!)
Another issue is that as we are dealing with a small population here (trans people make up under 1% of the US population, according to nearly all estimates) and certain subsets of this population, e.g. trans people who haven’t had medical transition or are currently going through it, are particularly hard to reach out to. This is especially true for specific topics like trans people in sports (miniscule number of trans athletes) and in the military, for example. This problem of a small population is usually bridged via convenience sampling and in general by recruiting small samples rather than going through the extra effort to get a large sample, but this also means that our samples are less useful overall. These sample issues can hopefully be avoided more in the future as more attention and funding goes towards studying trans issues. We should absolutely keep an eye out for newer, higher quality research as it comes out. In the meantime, we ought to work with the existing research and acknowledge the limitations that come with it.
Social Transition
Social Transition
Social transition improves depression, anxiety, and psychological function
- Journal of Adolescent Health: Connolly et al. 16
- Analyzes consensus on the effectiveness of social transition
- “Gender-affirming medical therapy and supported social transition in childhood have been shown to correlate with improved psychological functioning for gender-variant children and adolescents.”
- Journal of the American Academy of Child and Adolescent Psychiatry: Durwood et al. 17
-
Children who socially transition report levels of depression and anxiety which closely match levels reported by cisgender children, indicating social transition massively decreases the risk factor of both.
-
Puberty Blockers
Puberty Blockers
Puberty blockers are safe, well-studied, completely reversible, endorsed by credible medical and endocrinological associations, and effective at reducing dysphoria, anxiety, and depression.
- Public Broadcasting Service News: Korry 16
- Everything you need to know about puberty blockers
- Full-blown puberty is irreversible
- Taking a gonadotropin-releasing hormone (GnRH) agonist, secretion of the sex hormones can be stopped and the onset of puberty suppressed, so that the body does not develop secondary sex characteristics
- This has been done safely for decades to suppress sex hormones in children who develop too early, a condition known as precocious puberty. Suppressors have also been used to treat endometriosis, uterine fibroids and prostate cancer.
- It was only in 2008 that the Endocrine Society approved puberty suppressors as a treatment for transgender adolescents as young as 12 years old. The Society, with members in more than 100 countries, has since declared that the intervention appears to be safe and effective. In 2011 the World Professional Association for Transgender Health (WPATH), also issued Standards of Care for the treatment of patients with gender dysphoria, which include puberty suppression.
- Human Rights Campaign et al. 16
- BIG report on trans youth and transition
- Endorsed by the American Academy of Pediatrics & the American College of Osteopathic Pediatricians which affirms the validity of transgender youth, encourages appropriate care and respect for their transness and provides resouces on how to do so.
- Outlines TYPES OF TRANSITION: hormone blockers are the ONLY treatment used on adolescents and are COMPLETELY reversible.

- Karalexi et al. 20
- Study on the cognitive side-effects of puberty blockers
- “Current evidence does not support an adverse impact of gender-affirming hormone therapy on cognitive performance in birth-assigned either male or female transgender individuals”
- “An enhanced effect on visuospatial ability following post-pubertal hormone therapy was shown in assigned females”
- “Pooling data from cross-sectional studies showed a higher performance in verbal working memory in treated assigned males”
- Staphorsius et al. 15
- Study on the executive functioning side effects of puberty blockers
- “our results suggest that there are no detrimental effects of GnRHa on EF”
- “We found no significant effect of GnRHa on ToL performance scores”
- Endocrine Society Guidelines: Hebree et al 17
- A clinical practice guideline for puberty blockers
- “Puberty suppression typically relives distress for trans adolescents by halting progression of physical changes such as breast growth in trans males and voice deepening in trans females and is reversible in its effects”
- “Puberty suppression medication is reversible”
- van der Miesen et al. 20
- “Transgender adolescents show poorer psychological well-being before treatment but show similar or better psychological functioning compared with cisgender peers from the general population after the start of specialized transgender care involving puberty suppression.”
- De Vries et al. 11
- Compares psychological function before and after treatment with puberty blockers regarding 70 trans people
- “Behavioral and emotional problems and depressive symptoms decreased, while general functioning improved significantly during puberty suppression”
- Longer term study – looked at kids in 2000 and followed up in 2008
- Giordano et al. 20
- Article on why puberty blockers are prescribed and whether or not they are experimental.
- “Puberty delaying medications are currently provided off label to adolescents affected by gender dysphoria and this particular use cannot be investigated by a RCT. We have shown that this does not mean they are experimental drugs or are provided experimentally. Whether or not these (or even approved drugs) are ethically prescribed depends on whether they are likely to serve the patient’s health interests based on the evidence available at the time of prescription.”
- Hormone blockers are not new
- “Since the mid 1990s, puberty delaying medications have been prescribed to some adolescents (not prepubertal children) with severe and persistent gender dysphoria, in cases in which such distress was aggravated by pubertal development.”
- “The Royal College of Psychiatrists, in 1998, recommended delaying puberty in young adolescents who experienced strong and persistent ‘cross-sex identification’ and distress around the physical body that intensifies with the onset of puberty.”
- “Puberty blockers are not ‘novel’ treatment. They were recommended by prominent bodies of medical opinion in the UK and internationally over two decades ago, and have thus been part of standard medical treatment for many years.”
- “GnRHa has been used in the treatment of gender dysphoria since the mid 1990s, and their efficacy in delaying puberty in adolescents is documented by numerous studies and scientific publications” (21 scientific studies are then listed)
- Costa et al. 15
- Study of 201 kids between the ages of 12-17 with gender dysphoria
- Subjects were assessed for psychosocial functioning utilizing the Children’s Global Assessment Scale (CGAS), which indicated positive mental health outcomes after puberty suppression
- “The CGAS is one of the most widely used rating scales designed to measure how children and adolescents function psychosocially in daily life”
- “Results from this study indicate that psychological support is associated with a better psychosocial functioning in GD adolescents, especially if presenting psychological/psychiatric problems. Moreover, puberty suppression was associated with a further improvement in global functioning. Finally, global functioning improved steadily over time in GD adolescents receiving both psychological support and GnRHa [blockers]”
- Results also showed slightly higher CGAS scores for the sample group that was “immediately eligible” for puberty blockers compared to the “delayed eligible” group that only received psychological support, although with such a small sample size the researchers ultimately consider this difference negligible.
- A combination of these two approaches enabled subjects to reach levels of psychosocial functioning comparable to peers.
- de Waal et al. 06 (second link)
- Some guidelines towards gender dysphoria treatment, focusing on trans adolescents
- “Physical treatment outcome following interventions in adulthood is far less satisfactory than when treatment is started at an age at which secondary sex characteristics have not yet been (fully) developed”
- “Often have difficulties in connecting socially and romantically with peers while still in the undesired gender role, or the physical developments create an anxiety that limits their capacities to concentrate on other issues”
- “Suffering from gender dysphoria without being able to present socially in the desired social role, and/or to stop the development of secondary sex characteristics usually leads to problems in these areas”
- Giordano 08
- Paper focused strictly on the ethicality of puberty blockers
- Argues that the general improved quality of life, including substantially reduced risk of suicide, justifies the ofen challenged ethics of pubertal suppression.
- Endocrine Society 13
- Found that medical intervention in transgender adolescents appears to be safe and effective and that hormone treatment to halt puberty in adolescents with gender identity disorder does not cause lasting harm to their bones.
- Gallagher et al. 15
- Study on some commonly cited side effects of puberty blockers
- “Puberty was recovered within 1 year after GnRHa treatment discontinuation, and there were no abnormalities in reproductive function”
- “Bone mineral density decreases during GnRHa treatment but recovers to normal afterwards, and peak bone mass formation through bone mineral accretion during puberty is not affected”
- Neely EK et al. 10
- Assessment of the extent of puberty suppression during treatment
- ”During posttreatment follow-up (3.5 ± 2.2 years), all patients achieved a pubertal hormonal response within 1 year”
- “No impairment of reproductive function was observed at adulthood (mean age: 24.8 years)”
- “At callback of adult subjects we did not find impairment in reproductive function, consistent with previous studies”
- Heger et al. 06
- Study of reproductive function in AFAB subjects after GnRH puberty blocker treatment,
- ”Long-term GnRH agonist treatment for female central precocious puberty does not impair reproductive function”
- “None of the women who wanted to become pregnant, had to utilize assisted methods for inducing pregnancies”
- Magiakou et al. 09
- Further data on the effects of blockers on AFAB subjects
- ”Girls treated in childhood with GnRHa have normal BMI, BMD, body composition, and ovarian function in early adulthood”
- “There is no evidence that GnRHa treatment predisposes to polycystic ovary syndrome or menstrual irregularities”
- Pasquino et al. 08
- Further data on the effects of blockers on AFAB subjects
- “GnRHa treatment in ICPP is safe for the reproductive system, BMD, and BMI”
- “Menstrual pattern was normal. Six girls became pregnant and delivered normal offspring”
- “Hormonal values and ovarian and uterine dimensions, reduced during treatment, increased to normal after 1 yr without therapy”
- “At complete resumption of gonadal activity, mean BMD lumbar spine increased to 1.000 ± 0.11 g/cm2 , not significantly different from controls”
- Mean vBMD increased not significantly different from controls
- N Jay et al. 92
- Study evaluated the menstrual function of 46 girls with CPP who had been treated for at least 2 years with GnRHa and were up to 7 years post-treatment
- “Ovulation was demonstrated in 50% of the girls studied within 1 yr of menarche and in 90% of the girls studied 2 yr or more post-menarche, including 5 girls who reported pregnancies. The development of regular ovulatory menstrual function in these girls with CPP is in accord with previously documented patterns in normal adolescents”
- https://www.liebertpub.com/doi/full/10.1089/trgh.2015.0008
Common Puberty Blocker Myths:
Mostly taken from here
1. “Blockers are harmful to bone density”
The Endocrine Society found that medical intervention in transgender adolescents appears to be safe and effective and that hormone treatment to halt puberty in adolescents with gender identity disorder does not cause lasting harm to their bones.
Some meta-studies which show bone density and bone mineral density aren’t harmed:
2. “Young people wouldn’t want to take puberty blockers if they knew the risks”
Vrouenraets et al. 16 found that the few negative effects of puberty blockers do not change children’s minds and most adolescents stated that the lack of long-term data did not and would not stop them from wanting puberty suppression. They said that being happy in life was more important for them than any possible negative long-term consequence of puberty suppression.
3. “Puberty blockers will give trans kids osteoporosis and make them sterile”
Heger et al. 99 found that long term puberty blocker treatment of precocious puberty girls preserved genetic height potential and improved FH significantly combined with normal body proportions. No negative effect on bone mineral density and reproductive function was seen.
4. “Children are too young to know they are trans and are pushed to take blockers by parents / social media / peer pressure”
There are multiple accounts by parents and older trans people who observe that they/their child knew that they were transgender from a young age – Here is one such account and another article explaining how transgender kids aren’t rushed into transitioning. These kids seem to have a strong identity at a young age.
5. “It is not ethical to give puberty blockers to transgender children”
Focusing strictly on the ethicality of puberty blockers, Giordano argues that the general improved quality of life, including substantially reduced risk of suicide, outweighs the ethical considerations of disrupting puberty. Puberty blockers can be used to relieve stress from a patient and give them more time to get an accurate diagnosis of the situation, as was the case here - certainly more ethical to go forward with an accurate diagnosis than without one.
6. “The neutral decision is to not let minors access puberty blockers”
-
PHSA: Withholding puberty blockers and hormone therapy is not a neutral option and can result in an increased risk of mental health issues.
-
WPATH: Withholding puberty suppression and subsequent feminizing or masculinizing hormone therapy is not a neutral option for adolescents.
-
ASOCTG: Withholding of gender affirming treatment is not considered the neutral option, and may exacerbate distress in a number of ways including increasing depression, anxiety and suicidality, social withdrawal, as well as possibly increasing chances of young people illegally accessing medications.
-
The scottish gov say its not the neutral option “Withholding puberty blockers and hormone therapy is not a neutral option and can result in an increased risk of mental health issues”
Case Studies:
These case studies only focus on one person at a time. While they don’t have the statistical validity that a study would have at a larger sample size, it can give us qualitative insight into how these people experience what they go through.
- Kettenis et al. 11
- Dutch trans man who started on puberty blockers at age 13 in 1988. His health and well being was monitored regularly for over 22 years
- he was well-functioning with no clinical signs of a negative impact of earlier puberty suppression on brain development, metabolic and endocrine parameters, or bone mineral density
- Cohen-Kettenis 98
- Focuses on one person’s case in which puberty blockers were used at a young age to relieve pressure from them, give them more time to go through proper psychotherapy, and get a more reliable diagnosis of the situation
- Demonstrates that puberty blockers can be used to more to help more accurately diagnose gender dysphoria
- This should make puberty blockers an appealing option even to people who accept the science around being transgender but still believe that it’s mostly a trend
Prevalence of Discrimination
Prevalence of Discrimination
Discrimination against trans people is a real thing and is pervasive in many aspects of society. It’s not something that we can simply ignore when talking about trans people.
- European Union LGBT Survey 13
- LGBT folks’ self-reported perceptions of discrimination
- Regarding trans people, finds high levels of perceived discrimination across the board, including:
- 46% felt discriminated against or harassed within the past year for being trans
- 29% felt discriminated against when it came to looking for employment
- 70% hid being trans during schooling before becoming 18 years old
- Wittle et al. 07 (second link)
- Uses data from 872 respondents in the UK, which is a large number of respondents compared to most studies on trans people (pg 26)
- At the time, the most comprehensive study on discrimination of trans people (pg 17)
- There are a number of ‘trigger points’ at which trans people start being discriminated against during their transition, the most common of which is once they come out at work (pg 25-6)
- Aside from that, there’s a wide variety of ways and places in which trans people are discriminated against
- Uses data from 872 respondents in the UK, which is a large number of respondents compared to most studies on trans people (pg 26)
- Trans Employee Experiences Survey by TotalJobs 2016
- Survey of 432 transgender people living in the UK and Ireland, focused on their experiences of discrimination in the workplace. Methodology made it so that the people who were surveyed had transitioned specifically while working/actively seeking work
- Quantitative survey results came alongside qualitative ‘further comments’ by some respondents to better explain their experiences
- General trend in play in which most transgender employees received some support and acceptance, though with a substantial minority experiencing discrimination
- Most discrimination tended to come from fellow employees and customers, not so much management.
Impact of Discrimination
Impact of Discrimination
Suicidality is heavily influenced by bullying, discrimination, and poor treatment. Suicide attempt rates are also far higher among individuals who experience substantial discrimination or harrassment. The ~40% suicide attempt statistic is often misrepresented/misunderstood.
Let’s talk about the ~40% suicide statistic first.
What exactly is it referring to?
-
This number usually originates from the National Transgender Discrimination Survey**, which found that 41% of respondents had attempted suicide at some point in their lives. **The 41% statistic is one of a range of estimates. Some people will cite 41%, others 40%, others 50%. Different surveys and studies have gotten different results, with one review of 21 studies giving back a range between 32% and 50%.
-
This statistic is exclusive to trans people, not the LGBT community at large. The LGB population doesn’t suffer as much as the transgender population for a number of reasons, e.g. different levels of social acceptance and the additional healthcare burdens that trans people deal with.
-
The statistic refers specifically to suicide attempts, not completed suicides. This is important because very few suicide attempts actually result in a death. Estimates for the general population say that every 25 attempts results in 1 successful death, and every year around 285,000 people become new survivors of suicide. This means that anyone who conflates the 40% attempts statistic with deaths is accidentally inflating the suicide rate by 25x.
So how do people misuse it?
-
Some people will argue that the high suicide attempt rate means that being LGBT is unhealthy by its very nature, so we should discourage people from being transgender. This ‘discourage transness’ argument is contradicted by the very same surveys that found these high attempt rates, as shown in some of the below source annotations (tldr the same surveys that found 40% also found these numbers were higher for people who experienced more victimization, showing that affirmation rather than discrimination would be more helpful for these people). The ‘discourage transness’ argument also fails at a practical level insofar as curative therapy hasn’t shown itself to be effective yet, often causing more harm than good. This doc goes an extra step to show how affirmation, not discouragement, lowers suicide attempt rates.
-
Sometimes the argument made is that the high suicide attempt rate proves that transition doesn’t work. However, this statistic refers specifically to lifetime suicide attempts, which means that it’s possible most of those suicide attempts could have happened in life before any transition took place. If we saw a large number of suicide attempts before transition but much fewer after transition, that would directly contradict the argument being made. Regardless, people making this argument usually fail to actually substantiate any causal connection for transition causing suicides.
An extra bit on calculating successful suicide rates:
- Getting data on suicide attempts (attempting and failing to kill yourself) is much easier to do than getting data on successful suicides (attempting and succeeding). This is for a number of reasons:
- People who attempted but didn’t succeed with a suicide are still alive and thus can be surveyed, so you can reach out to these people and ask about past suicide attempts. You can’t survey people who are dead from suicide.
- Long-term follow-ups are crucial to understanding successful suicide rates, but long-term follow-ups in general have been harder to come across in the literature on transgender issues, and conducting long-term follow-ups for this population has proven difficult. However, you only need a one-time survey to learn about previous suicide attempts from people who are still alive.
- It’s next to impossible to gather data on people who believed they were trans but committed suicide before coming out to anyone.
- Sometimes transgender people commit suicide but due to a lack of an easily-identifiable paper trail on them being transgender (e.g. legal documents weren’t changed to reflect their transgender identity), it’s harder for researchers to identify trans people who committed suicide.
- Nevertheless, some work has been done to get a better idea of the successful suicide rate. This study published in 2020 followed 8,263 Dutch transgender people over a long period of time, and it found a suicide rate of 0.6% (buried in the study though, see table 1). This is obviously a far cry from 40% but is still around 4x higher than the suicide rate of the general Dutch population (the study looked at people who went to an Amsterdam clinic).
Annotated sources:
- National Transgender Discrimination Survey: Grant et al. 11
- MASSIVE survey of 6,450 trans people
- 41% of respondents reported attempting suicide compared to 1.6% of the general population
- These rates rose for those who:
- lost a job due to bias (55%)
- were harassed/bullied in school (51%)
- had low household income
- were the victim of physical assault (61%)
- were the victim or sexual assault (64%)
- Virupaksha et al. 16
- Broad meta-analysis of 21 studies on the trans suicide attempt rate (it’s quite high).
- The suicide attempt rate ranges from 32% to 50% across countries
- The following were found to have an impact on the suicide attempt rate
- Gender-based victimization
- Discrimination
- Bullying
- Violence
- being rejected by the family, friends, and community
- harassment by intimate partner, family members, police and public
- discrimination and ill treatment at health-care system
- Zeluf 18
- Swedish study on trans sucide prevention
- 37% of respondents reported that they have seriously considered suicide during the past 12 months and 32% had ever attempted a suicide
- Suicide ideation is assiated with:
- Offensive treatment
- lifetime exposure to trans-related violence
- less satisfaction with contacts with friends and acquaintances and with one’s own psychological wellbeing
- lack of practical support
- Williams Institute: Haas et al. 14
- Massive demographic analysis which codifies the many social & institutional factors which contribute to trans suicide rates
- Prevalence of suicide attempts is elevated among those who:
- disclose to everyone that they are transgender or gender-non-conforming (50%)
- among those that report others can tell always (42%) or most of the time (45%) that they are transgender or gender non-conforming
- The suicide attempt rate was associated with mental health factors and experiences of:
- Harassment
- Discrimination
- Violence
- Rejection
- Williams Institute: Herman et al. 19
- Discrimination or mistreatment in education, employment, housing, health care, in places of public accommodations, or from law enforcement is associated with higher prevalence of suicide thoughts and attempts (13.4% compared to 6.3%)
- Those who reported that their spouses, partners, or children rejected them because they are transgender reported higher prevalence of lifetime and past-year suicide attempts (10.5% compared to 5.1%)
- Respondents who had been rejected by their religious communities or had undergone conversion therapy were more likely to report suicide thoughts and attempts (13.1% compared to 6.3%)
- People who are not viewed by others as transgender and those who do not disclose to others that they are transgender reported lower prevalence of suicide thoughts and attempts (6.3% compared to 12.2%)
- The cumulative effect of minority stress is associated with higher prevalence of suicidality. For instance, 97.7 percent of those who had experienced four discriminatory or violence experiences in the past year (being fired or forced to resign from a job, eviction, experiencing homelessness, and physical attack) reported seriously thinking about suicide in the past year and 51.2 percent made a suicide attempt in the past year.
- Klein and Golub 16
- Family rejection linked to suicide, drug use, and overall detriments to health
- To cope with transgender-related discrimination:
- 42.3% of the sample reported a suicide attempt
- 26.3% reported misusing drugs or alcohol
- “After controlling for age, race/ethnicity, sex assigned at birth, binary gender identity, income, education, and employment status, family rejection was associated with increased odds of both behaviors. Odds increased significantly with increasing levels of family rejection.”
- Adams et al. 19
- SITBs (suicidal thoughts and behaviors), among the transgender population, are both universally high and impacted by race/ethnicity, educational attainment, and income
- Lifetime suicidal ideation was reported in 34 studies and attempts in 46 studies
- “The myth that transition leads to SITBs continues to be used to deny transgender health care access and legislative rights, despite a lack of empirical support for this position and repeated research debunking it”
- Williams institute: Herman et al. 19
- “A lower proportion of respondents who lived in a state with a gender identity nondiscrimination statute reported past-year suicide thoughts and attempts than those who lived in states without such a statute”
- “discrimination against transgender people in employment, housing, and public accommodations.34 By providing at least some level of protection against discrimination based on gender identity, state nondiscrimination policies are thought to enhance the health and well-being of transgender people.”
-
https://www.huffpost.com/entry/the-truth-about-transgend_b_8564834
-
[https://www.tandfonline.com/doi/full/10.1080/00918369.2011.534038]https://www.tandfonline.com/doi/full/10.1080/00918369.2011.534038)
-
https://www.rondpointdelitinerance.ca/blog/infographic-wednesday-preventing-tragedy-lgbtq-youth-homelessness (so sorry some of it is french)
-
https://www.lgbtmap.org/news/understanding-transgender-issues-unfair-price-release
- https://jamanetwork.com/journals/jamapediatrics/fullarticle/2704490
Impact of Social/Familial Support
Impact of Social/Familial Support
Family support decreases suicide attempts and drug usage while improving the mental health of trans people.
- American Academy of Pediatrics: Olson et al. 16 (cited)
- Socially transitioned transgender children who are supported in their gender identity have:
- Normative levels of depression
- Minimal elevations in anxiety
- Lower rates of internalizing psychopathology (a spectrum of conditions characterized by negative emotion) then non-socially transitioned people
- Socially transitioned transgender children who are supported in their gender identity have:
- Trujillo et al. 17
- Helping trans individuals cope with harassment and rejection, particularly by drawing on social support, may promote better mental health, which could help reduce suicidality in this population.
- Cornell University
- A literature compilation of the findings of 42 peer-reviewed studies that analyzed the links between family support and the health and well-being of LGBT youth
- 25 studies found that accepting behavior by parents toward their children’s sexual orientation or gender identity is linked to the health and well-being of LGBT youth.
- The other 17 studies found that family support in general (i.e. not necessarily in response to children’s sexual orientation or gender identity) is linked to the health and well-being of LGBT youth.
- This compilation might suffer from similar problems as the Cornell link in the [Medical Transition] section. Things to consider
- A literature compilation of the findings of 42 peer-reviewed studies that analyzed the links between family support and the health and well-being of LGBT youth
- Trans PULSE (subsidiary of the Canadian Institutes of Health Research)
- From Ontario (not international scope) but academically credible and VERY widely cited
- Analysis of the ways in which parental support affect elements of disadvantage experienced by transgender youth.
- Strong parental support decreases the likelihood of a suicide attempt within the past year from 57% to just 4%.
- Bauer et al. 15
- Data from trans people age 16+ in Ontario, Canada, including 380 who reported on suicide outcomes
- “Interventions to increase social inclusion and access to medical transition, and to reduce transphobia, have the potential to contribute to substantial reductions in the extremely high prevalences of suicide ideation and attempts within trans populations”
- Shows every step of transitioning from changing legal documents to surgeries lowers suicide risk more
- Başar et al. 16
- “Social support from family was associated with better QoL in psychological QoL, whereas perceived support from friends significantly predicted all other domains of QoL”
- “strategies to improve and strengthen friend and family support for individuals with GD should be explored by clinicians”
- “Social support and discrimination were found to have opposing contributions to QoL”
- N = 94, median age = 26
Chosen Name/Pronoun Usage
Chosen Name/Pronoun Usage
The use of trans people’s chosen name decreases suicide ideation, severe depression, and suicide attempts
- Journal of Adolescent Health: Russell ST, et al. 18 (cited)
- Compared to those without chosen name usage, trans people with chosen name usage experienced:
- 71% drop in severe depression
- 34% drop suicidal ideation
- 65% drop in suicide attempts
- Keep in mind that as of 2020, this is the only study available on chosen name usage specifically
- Compared to those without chosen name usage, trans people with chosen name usage experienced:
Some additional notes:
- If someone were to adopt children, there’s no biological basis for calling them that kid’s parent, because they’re not biologically related. However, there is a social reason and a legal reason to call them that kid’s parent – functionally, they serve the same purpose as any other parent would, so it makes much more sense to call them parents than it does to call them glorified child buyers. Similarly, it doesn’t make sense to use he/him pronouns on a trans woman, nor vice versa. If the trans person identifies and passes as being a certain gender, they ought to be treated with the respective pronouns. In most contexts, the ‘trans-cis’ distinction will be about as relevant as the biological-adopted distinction with parents.
- “You don’t have to call someone by their preferred pronouns.” Yeah and you don’t have to flush your poop down the toilet after shitting in a public restroom but it’s a respectful thing to do.
Bathroom Bills
Bathroom Bills
Evidence for the public safety argument in regards to bathroom bills is unsubstantiated in data. Bathroom bills would give rise to other problems which proponents leave unaddressed as well. Also, check out this resource for additional material on the subject.
- Hasenbush et al. 19
- Analysis of crime & privacy violations in Massachusetts as they relate to concerns raised by those who advocate for ‘trans bathroom bills’
- Analysis indicates there is no empirical evidence to support these concerns; such crimes & privacy violations are exceedingly rare.
- Calls for trans bathroom bills are fearmongering, plain and simple.
- To add additional context in the case of Massachusetts, a different study sampled 452 transgender people in Massachusetts and found that 65% of respondents experienced discrimination/harassment in public accomodations, part of which includes discrimination in bathrooms. This is in spite of the limited anti-discrimination laws that exist in the state. This would suggest that in Massachusetts, it would be more productive to focus on transgender discrimination than it would be to block them from certain restrooms.
- Bianco 15
- Zero reported cases of transgender people harrassing cisgender people in the bathroom, according to multiple organizations
- Experts agree that bathroom bills are unsubstantiated and driven by fearmongering
- Suggests that bathroom bills perpetuate violence against transgender people by placing them in discriminatory situations
- British Social Attitudes: Swales & Attar Taylor 17
- Regardless of baseless fear mongering, most people in the UK are fine with transitioned transgenders using the restroom of their gender -* “Women tend to be more comfortable with this than men, with 72% of women saying they are “very” or “quite comfortable” with a transgender woman using a female toilet, compared with 64% of men saying they are comfortable with a transgender man using male toilets. Around 1 in 6 (14% of women, and 15% of men) say they are not comfortable with this.” (pg 14)
- This one excludes the “Neither comfortable nor uncomfortable” answer which was another 14% from the 2017 survey
- Charlotte Observer 16
- Even after searching for hours through dozens of alleged instances of transgender bathroom incidents, only 3 were able to be verified that had occurred since 1999
- Seelman 16
- Uses data from the National Transgender Discrimination Survey, looking specifically at trans people in college
- After controlling for interpersonal victimization, found that denying access to desired bathroom increases suicidality of trans people
- NTF 18
- Consensus of anti sexual assault and domestic abuse charities in the United States that supports trans inclusive bathroom policies
- Police Foundation 17 (pdf)
- Analyzed police reports of sexual assaults in Atlanta, Dallas, Miami Beach, Miami Gardens, and Tucson before and after each city passed a non-discrimination policy for LGBT people
- After looking over years worth of relevant data, they were unable to find any evidence of a man disguising as a woman to go into a women’s restroom and sexually harass women
- Murchison et al. 19
- When forced to use the bathroom correlated with assigned sex there was an increase prevalence of sexual assaults which trans people experienced compared to their cis counterparts
- 26.5% more among transgender boys
- 27.0% more among nonbinary youth assigned female at birth
- 18.5% more among transgender girls
- 17.6% more among nonbinary youth assigned male at birth
- When forced to use the bathroom correlated with assigned sex there was an increase prevalence of sexual assaults which trans people experienced compared to their cis counterparts
-
https://williamsinstitute.law.ucla.edu/publications/gendered-restrooms-minority-stress/
- https://www.hsph.harvard.edu/news/hsph-in-the-news/transgender-teens-restricted-bathroom-access-sexual-assault/
Specific Debunks:
Keep in mind that singular incidents don’t actually prove a broader statistical trend, nor do small compilations of incidents.
- Colorado high school incident - claimed that a trans woman was harassing other girls in a high school bathroom
- Debunk - an interview with the school’s superintendent confirms that this never happened
- Joey Salads experiment - Salads dresses up how he thinks a trans woman would, and goes into a women’s restroom, receiving negative responses from others in the scene
- Video Debunk
- Salads misrepresented the behaviour of trans women and used a single-person restroom, so his whole experiment was probably staged. A replication of the experiment got no negative responses from others in the scene
- Dallas incident - Trans woman allegedly taking photos of children in women’s restrooms
- Debunk - the website’s about page says “And here we are today, to bring you nothing but pure horse shit… This should go without saying, but everything on this website is purely for entertainment purposes. We are in no way affiliated, or trying to look like we are affiliated with any local news station.”
- Casper, Wyoming incident - Trans woman, Michelle Martinez, sexually molested 10 yr-old
- This actually did happen, but this one incident can’t be extrapolated onto the greater trans population, especially not with the existing empirical evidence regarding bathroom bills
- This one also happened in a private restroom in someone’s home, so that wouldn’t have been covered by a restrictive bathroom bill anyway as private household bathrooms aren’t segregated by gender.
- Family Research Council compilation - cites 25 instances of men going into female bathrooms
- Most if not all of the stories they cite do NOT involve or even MENTION trans people; this is by-and-large a compilation of CIS men harrassing women
- While the FRC argues that the problem itself is in fact cis men exploiting a perceived loophole, most of their “examples” lack any connection to bathroom bills regardless.
- Even if every single incident involved a trans person, this does barely anything to justify bathroom bills. 25 instances over the course of 18 years (1999-2017) is barely anything demonstrative of a larger problem in need of being addressed at a large scale.
- Most, if not all, of those incidents would be illegal even without a restrictive trans bathroom bill being in effect, so introducing such a law isn’t really the solution here.
- Gathering this sort of data via media reports is rather dubious too, considering some of these incidents go unreported and some of those which are reported turn out to be hoaxes. It doesn’t help that a good few hyperpartisan and anti-trans advocacy groups are cited, like The Daily Wire and MassResistance, which both have interest in spreading anti-trans info even if it turns out to be misleading or falsified.
- Most if not all of the stories they cite do NOT involve or even MENTION trans people; this is by-and-large a compilation of CIS men harrassing women
- “When is 90% not Substantially ALL?” - TERF wordpress blog
- Ignoring the preamble, the post is very obviously a gish gallop which has lot of dead links and an awful lot of links unrelated to the transgender bathroom stuff. The compilation also includes way more than just transgender people, extending its focus to cross-dressers (that is, anyone who is wearing literally any clothing which we associate with the opposite gender, such as a naked man who is wearing nothing but women’s heels).
- Many of these incidents don’t even give us evidence that cross-dressing is something the people involved do on a regular basis, e.g. an incident where a man impersonated a female police officer. We don’t know if that person regularly cross-dresses or if the person was impersonating a police officer who just happens to be a woman, but it gets included in the blog’s list anyway.
- The blog even includes incidents where no crime was committed, e.g. a man who drowned because the skirt he was wearing was too tight to let him swim. How is this an example of a transgender sex crime in a bathroom??
Other Notes:
- If a man wanted to pretend to be trans as an excuse to rape women, he doesn’t have to fake being a woman to go into the bathroom. The law won’t physically prevent him from going in there.
- Rape, sexual harassment, and voyeurism are already illegal, so if your primary concern is women being sexually harassed or raped by men in the bathroom, then there’s already laws to address your concerns.
- Even from a conservative perspective, bathroom bills give an unnecessary amount of power to big government and aren’t necessarily effective. It’s not practical for the government to enforce a trans-oriented policy like this because most trans people don’t look like their birth sex. The cis man won’t present as a woman, just as a trans man wouldn’t present as a woman. That would make it look like a girl is going into the men’s restroom, or vice versa - memes like this and this carry home the point.
- The burden of proof that transphobes for stuff like this can easily be turned against them. Someone could find several instances of cis people harrassing trans people in bathrooms (which is far more common anyway) but that doesn’t justify banning cis people from their respective bathrooms.
- You don’t want to ask “find me one instance of a bathroom assault”, as you can find one instance of all sorts of unusual things. It’s instead better to ask “show me the statistical trends on bathroom sexual assault” as that information is infinitely more useful when talking about broader societal issues.
{kind=link}
{kind=link}
Prisons
Prisons
- Just Detention International Organization 13
- 59 percent of transgender women housed in men’s prisons had been sexually abused while incarcerated, as compared to 4 percent of non-transgender inmates in men’s prisons
- https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/567053/prisoner-transgender-statistics-march-april-2016.pdf
- “Based on this exercise, there were 0.8 transgender prisoners reported per 1,000 prisoners in custody.”
- That translates to around 1/1250 prison inmates being trans, and 0.08% is well below the typical 0.6% general population estimate for transgender people.
- https://transequality.org/blog/federal-survey-40-of-transgender-prisoners-are-sexually-abused-each-year
Public Perception and Depiction
Public Perception and Depiction
In media, trans and LGBT people are generally depicted either negatively or in shallow, stereotypical ways. Polling usually shows a substantial minority who oppose trans-affirming policies, though fortunately most Americans are fine with trans people.
- Colorado State University: Matthews 16
- Interesting (and long) qualitative analysis on the depiction of transgender people in Sports Illustrated over past decades.
- Finds disproportionately negative depictions (of course).
- McInroy 16
- Finds that LGBT folk are usually depicted in media in stereotypical ways, which could limit their perception of their possible future
- Hughto et al. 20
- frequent exposure to negative depictions of transgender people in the media was significantly associated with clinical symptoms of depression, anxiety, global psychological distress, and post-traumatic stress disorder (PTSD) in this population
- those who reported greater frequency of exposure to these messages were significantly more likely to exhibit clinical symptoms of depression, anxiety, global psychological distress, and PTSD. The association held even after adjustments were made for variables such as age, race, income, and reported experiences of childhood and/or adult sexual or physical abuse, which suggests that negative media messages may have an independent impact on the mental health of transgender populations exposed to such messages.
- UCLA Williams Institute: Luhur, Brown, & Flores 17
- While a majority of Americans agree on giving a number of rights to trans people, there is still a substantial minority who oppose such
- While a majority of Americans agree on giving a number of rights to trans people, there is still a substantial minority who oppose such
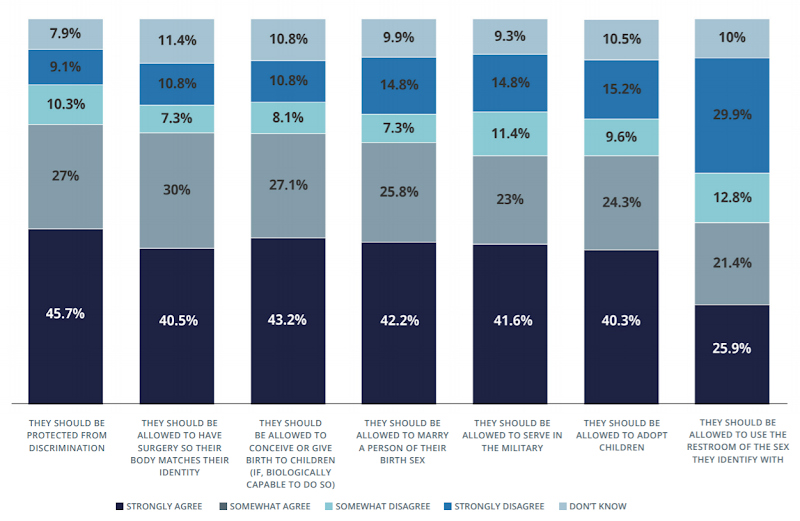
- YouGov 19
- A majority of Americans support a number of trans-affirming rights and policies, but there’s still some divide in places and a substantial opposing minority for nearly every related issue
- https://www.tandfonline.com/doi/full/10.1080/19359705.2013.777007
Trans Athletes
Trans Athletes
Trans athletes are at no significant advantage in athletics, especially since hormones reverse any strength discrepancies, yet face substantial discrimination in athletics. Keep in mind that specific instances of trans people winning sports competitions doesn’t actually prove anything about broader trends. Also worth noting the low quality of much of this research because there’s very few trans athletes and nobody cared about this until like 2015, which means we should be open to new research developments for this topic and a lot isn’t settled science yet
- Jones et al. 17
- Systemic review covering prior research on trans individuals’ performance in sports and preexisting sports policies concerning trans people, amounting to 8 research articles and 31 sports policies
- Finds that “There is no direct or consistent research suggesting transgender female individuals (or male individuals) have an athletic advantage at any stage of their transition”
- (includes cross-sex hormones, gender-confirming surgery)
- This particular subject is in need of more and better research because most research is really low quality, so using this systemic review as a definitive statement on the topic is a dumb thing to do. The systemic review is only as good as the studies it rests on.
- Much of the low-quality problem comes from small sample sizes (you can see sample sizes in this table). It’s hard to gather a large group of transgender athletes if there are so few in the first place. To put this into broader context, we are looking at a small portion of the population (trans people), within that group is a small number of athletes, and within that group we have trans athletes who do competitive sports, aka the people we can recruit for our sample. So we’re looking at a fraction of a fraction of a fraction of the population.
- Because of the lack of good research on the subject, anti-trans sports policies are likely based on little if any empirical evidence (very little of that evidence exists).
- Trans individuals experience substantial discrimination from sports institutions due to existing anti-trans policies.
- https://link.springer.com/article/10.1007/s40279-020-01324-6 Richardson and Chen published a critique of this study, this links to a rebuttal of the critique
- National Collegiate Athletic Association: Griffin et al. 10
- “Any athletic advantages a transgender girl or woman arguably may have as a result of her prior testosterone levels dissipate after about one year of estrogen therapy”
- “According to medical experts on this issue, the assumption that a transgender girl or woman competing on a women’s team would have a competitive advantage outside the range of performance and competitive advantage or disadvantage that already exists among female athletes is not supported by evidence.”
- National Collegiate Athletic Association: Board of Governors Statement on Transgender Participation (2021) with an associated policy pdf
- Very clear emphasis on maximizing both inclusiveness and fairness for athletes
- Only restriction in place for trans people is testosterone suppression treatment for transgender women - this policy is meant to preserve fairness in competition while letting trans women participate in their proper sports teams.
- The policy pdf goes more in-depth about broader inclusion of trans athletes into sports teams, suggesting ‘best practices’ for athletics administrators, coaches, etc. That mostly just comes down to standardizing NCAA practice at other schools, educating about non-discrimination laws that apply for sports, and being respectful and understanding towards trans athletes (sportsmanship!)
- University of Leicester: Hargie et al. 15
- “It is primarily the lack of public understanding regarding transgender people that remains the greatest cause of their exclusion”, not some preceived advantage among athletes.
- The study found interconnecting themes among all its participants to substantiate the prominence of public exclusion:
- the impact of alienating sports experiences at school
- the intimidating nature of the changing room environment
- the fear of public space and how this drastically constrained their ability to engage in sport and physical activity
- the overall impact of their exclusion in terms of being denied the social, health and well-being aspects of sport
- Lenzi 18
- Legal analysis about the legality of transgender sports policy in the context of Title IX and the 14th Amendment
- Broad conclusion in favor of inclusive policy for trans people, some nuance.
- There’s different types of trans-affirmative sports policies. States like Connecticut have a fully inclusive policy that lets you participate in whatever team aligns with your gender identity. The assumption here is that the very small number of transgender athletes doesn’t pose a significant threat to fairness for cis people. Other states like Idaho and Ohio have a partially inclusive policy which basically lets you participate in the team of your gender identity as long as you complete a year of hormone therapy. This restriction is meant to keep sports fair for everyone involved by dealing with biological advantages one group might have over the other.
- It’s important to note that this conclusion is primarily drawn from legal analysis, working its way through the existing law apparatus that we have in place. This is meant to provide a solution for trans athletes that is legal, so the legal prioritization might not be best for a debate about something else, e.g. the morality or impact of these policies.
- Throughout the paper Lenzi emphasizes that sex-segregated sports gives cis women a fair chance at being competitive against cis men, as cis men generally have a biological advantage. However, trans people who have gone through cross-gender hormone therapy are not comparable to their cis counterparts in the same way.
- “Before high school athletic associations devise regulations regarding transgender athletes, they must openly acknowledge the inherent biological differences between males and females. A trans girl, who has a male body that regularly produces testosterone, has a physical advantage over a cis girl whose body produces significantly less testosterone. However, when a trans girl receives cross-gender hormone therapy, the treatments greatly reduce any former biological edge. Hormone treatments for MTF trans girls increase body fat, decrease muscle mass, and may even cause a slight loss in height. After only one year of cross-gender hormone therapy, a trans girl will have estrogen and testosterone levels similar to the average cis girl.”
- https://theestablishment.co/no-female-trans-athletes-do-not-have-unfair-advantages-14b8e249f93c/
- This op-ed specifically focuses on the impact of HRT on trans people’s athletic performance, but from a qualitative POV - a trans woman explaining the experience she went through with HRT impacting her athletic ability
- This qualitative focus can give us a good perspective on what these trans athletes are going through when they go through HRT
-
https://drive.google.com/file/d/14Osr1FgL93AOAT7qve72NCR1TUnee96I/view
- https://www.youtube.com/watch?v=P6HbxVJlc4s
Other Notes:
On physiological differences: segregating sports based on something like height, testosterone, etc can get really messy especially when it’s tied in with the existing sex-segregation in sports. In some cases, this has led to the outright exclusion of biological females from women’s sports simply due to naturally high testosterone levels. Some of these policies need to be carefully thought through so as not to accidentally exclude people who really didn’t do anything to deserve it.
On Fallon Fox/Tamika Brents: For one, their specific match is pretty much just one match, one data point out of so many other matches and games. This one anecdote is not statistical data and is not generalizable to all trans people in sports (though let’s be real, finding any good statistical data on trans athletes is a challenge). Second, however shocking the concussion and broken skull were, these sorts of traumatic head injuries are sadly very common in MMA fighting, to the point where it’s even been banned in some countries (plus banned and relegalized in others). MMA is a relatively dangerous sport and Tamika Brents’ injuries are unfortunately not particularly out of the ordinary for that sport, so it doesn’t make much sense to hyperfocus on Fox being trans here.
On general “fairness” args: The pretty obvious rebuttal is that sex segregated sports does not somehow make everything fair. Some of this is more general (not all players of the same sex have the same testosterone levels) and some of it is specific to the sport (in basketball, taller players have an obvious advantage over shorter players). In the case of basketball, someone who is 6’4” in height has an obvious biological advantage over someone who is 5’4”, however we allow these two players to compete together while a typical cis man is barred from competing with a typical cis woman because of the man’s biological advantages. The question then comes down to what sort of fairness we want to promote, and for who, as different people benefit from different approaches to fairness in sports. This article covers the broader point fairly well.
Neurology/Biology
Neurology/Biology
Some trans individuals neurologically reflect cisgender people of their desired gender, suggesting a neurological component to their experiences. This suggests that gender has some biological basis, but not necessarily that gender is 100% biological. There’s obviously a sociological basis to gender and gender roles which complement its biological aspects.
- European Society of Endocrinology 18
- Brain Scans show that (many) transgender individuals neurologically reflect their identity, not their assigned gender at birth.
- The study included both adolescent boys and girls with gender dysphoria and used magnetic resonance imaging (MRI) scans to assess brain activation patterns in response to a pheromone known to produce gender-specific activity.
- The pattern of brain activation in both transgender adolescent boys and girls more closely resembled that of non-transgender boys and girls of their desired gender.
- Brain Scans show that (many) transgender individuals neurologically reflect their identity, not their assigned gender at birth.
- Smith et al. 15
- Out of 14 studies of brain structure (total N=307, N MtF=195, N FtM=112) with a total of 23 results: 6 results that trans people had brain structure similarities to their birth sex, 12 results that trans people had brain structure similarities to their gender identity, and 5 results that unclear results (either no significant sex differences or no significant differences between trans and cis participants, or both).
- 12 of 18 (66%) results with clear results suggest trans people have brain structures with similarities to their current gender identity.
- Keep in mind that’s no consensus, but it suggests there could be something to check out there
- Suraswat et al. 15
- Studies on gray matter, white matter, twins, and prenatal exposure all suggest – albeit, with limited sample sizes and methods – that transgender identity, like homosexuality, has a biological origin
- “Although the mechanisms remain to be determined, there is strong support in the literature for a biologic basis of gender identity.”
- “Current data suggest a biologic etiology for transgender identity. Studies of DSD patients and neuroanatomical studies provide the strongest evidence for the organic basis of transgender identity. Because the sample sizes of most studies on this subject were small, the conclusions must be interpreted with caution. Further research is required to assign specific biologic mechanisms for gender identity.”
- A highly source filled review article published by Harvard University on the biology of being transgender with also some very informative diagrams. Here are the studies on transgender biology mentioned there which the article itself goes into detail:
-
brain size accounts for some sex differences - https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3867125/; hormones change some of the aforementioned minor differences - https://pubmed.ncbi.nlm.nih.gov/27744092/; cis women with PCOS have some of the same differences trans women do - https://academic.oup.com/humrep/article/28/10/2832/622588; some stuff about how sexually dimorphic traits are better associated with specific hormone exposure and sexuality - https://en.wikipedia.org/wiki/Neuroscience_and_sexual_orientation; and something else I found while searching for the other details, which is that if we look at functional similarities rather than just structural ones, trans brains are more like the desired gender - https://health.clevelandclinic.org/research-on-the-transgender-brain-what-you-should-know
-
https://sillyolyou.wordpress.com/2019/05/16/the-illusion-of-neurosex-your-brain-is-not-male-nor-female/ This source argues that the brain is not truly ‘male’ nor ‘female’ and that the dichotomy doesn’t make much sense in the context of neuroscience
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4987404/
Detransition/Regret
Detransition/Regret
Detransitioning is rare in the first place, and when it does happen it is overwhelmingly driven by various forms of discrimination, not uncertainty with regards to identity. Regret rates (distinct from detransition rates) are also very low. This seems to be true for both trans adults and trans kids. Credit for most of this stuff goes to this doc by u/Albamc35, feel free to cite it for convenience. This resource from GenderGP is also a helpful resource.
Trans Kids Detransition:
-
Using information from the Australian Court, 96% of all patients who were assessed and received a diagnosis of Gender Dysphoria by the 5th intervenor (the Royal Children’s Hospital) from 2003 to 2017 continued to identify as transgender or gender diverse into late adolescence. No patient who had commenced stage 2 treatment had sought to transition back to their birth assigned sex.
-
A summarisation on all people treated in Amsterdam from 1972 up to 2015, which treats more than 95% of the transgender population in the Netherlands, found that out of those referred to the clinic in before the age of 18 and treated with puberty blockers, 4 out of 207 trans girls (2%) stopped puberty suppression without proceeding to HRT and 2 out of 370 trans boys (less than 1%) stopped puberty suppression without proceeding to HRT
-
A study of 143 youth receiving puberty-blocking medication in the Netherlands found that 3.5% chose to discontinue puberty blockers without seeking any further transition treatment.
-
A William’s Institute report finds that there is no significant difference between the number of trans teens and the number of trans adults (0.7% and 0.6% respectively). The slight decrease in the older age groups could be down to rejection from peers, as older generations are much less likely to support trans rights than younger people.
-
A study published in 2022 conducted a long-term followup of 317 trans kids and found that over the course of 5 years, a resounding 94% of kids kept their trans identity. Only 2.5% detransitioned back to a cisgender identity.
Also, trans kids are not ‘going through a phase.’ First of all, an article from a magazine from the American Academy of Pediatrics mentions how by age 4, children have a ‘stable sense of their gender identity.’ And a study on trans and cis kids (citied in this Forbes article) found gender identity — the concept of knowing whether one’s self is male, female or non-binary — is as strong in trans kids as it is among those identifying as cis. Similar results are found in this study.
General Detransition:
- A study on detransition rates in a national UK Gender Identity Clinic (pg 139) found out that of the 3398 patients who had appointments during this period, 16 (0.47%) expressed transition-related regret or de-transitioned. Of these 16, one patient expressed regret but was not considering detransitioning, two had expressed regret and were considering detransitioning, three had detransitioned, and ten had detransitioned temporarily.
- The reasons stated by patients for their regret or detransition included: social factors, reporting physical complications, and changing their mind about their gender identity and identifying as their gender assigned at birth, which shows that of that minority, alot were not due to releasing they are not trans
-
A transgender mental health survey in the UK (pg 66-67) found in terms of social changes that they had made in relation to being trans or transitioning, only 9% had significant regrets. In regards to the physical changes of being trans, only 2% having major regrets. Remember that regrets =/= detransition though
- A massive survey of trans people in the United States (pg 111) found that even including people who only temporarily detransition either socially or medical (or both), only 8% of respondents reported having de-transitioned at some point.
- Of these “detransitioners,” only 5% did it because they realized it was not for them, accounting for a mere 0.4% of the overall sample.
- And even then, 62% of those who had de-transitioned reported that they were currently living full time in a gender different compared to the gender they were thought to be at birth.
- “The 2015 U.S. Transgender Survey (USTS) is the largest survey examining the experiences of transgender people in the United States, with 27,715 respondents from all fifty states, the District of Columbia, American Samoa, Guam, Puerto Rico, and U.S. military bases overseas”
- Turban et al. 19
- Research on 27,715 transgender adults living in the US, 3,869 of whom had been exposed to gender identity conversion efforts
- They found that quote “exposure to [gender identity conversion efforts] before age 10 years was significantly associated with several measures of suicidality, including lifetime suicide attempts”.
- They also found no significant difference when comparing religious or secular conversion attempts. So it’s not a case of finding the right way to do it, there is no right way to do it.
- https://www.researchgate.net/publication/343775702_Detransition_rates_in_a_large_national_gender_identity_clinic_in_the_UK
SRS Detransition:
-
A study on people who went through sex reassignment surgery in the Netherlands found that of 162 trans adults, only 1 reported they would choose not to transition again. Another had some regrets but would choose to transition again (0.6% regret rate)
-
An analysis of all applications for sex reassignment surgery in Sweden found that of people undergoing SRS, regret was about 2.2% and there was a significant decline of regret over time
- In this international survey of 46 surgeons (67% of providers have been in practice for greater than 10 years) they were asked to select a range representing the number of transgender patients they have surgically treated, and this amounted to a cumulative number of approximately 22,725 patients treated by the cohort.
- 49% of respondents had never encountered a patient who regretted their gender transition or were seeking detransition care. 12 providers encountered 1 patient with regret and the rest encountered more than one patient. This amounted to a total of 62 patients. There were 13 patients who regretted chest surgery and 45 patients who regretted genital surgery.
- Overall, only 22 patients (0.1% of the sample) detransitioned because of a change in gender identity
-
A study on 232 trans women who were operated by the same surgeon ‘using a consistent technique’ found that none reported outright regret and only a few expressed even occasional regret. Dissatisfaction was most strongly associated with unsatisfactory physical and functional results of surgery.
-
An international study on 201 people who had trans-related surgeries found that postoperative satisfaction was 94% to 100%, depending on the type of surgery performed. Only eight (6%) of the participants reported dissatisfaction and/or regret.
-
A study in Belgium of 107 people who underwent SRS found none of the patients regretted their surgery.
-
A study of 218 patients in Sweden found only 3.8% had regretted it. The study also notes that support from family and friends is a huge factor in reducing regret. Keep in mind that this data was taken in 1998 during a time in which being trans was less socially accepted than they are now, so that number has evidently decreased over time
-
A study on 66 patients found none of the present patients claimed to regret their decision to undergo gender-transformation surgery.
-
A meta analysis, which looked at 74 follow-up studies and 8 reviews of outcome studies, found over a 30 year period, only 20 MTF and 5 FTM regretted transitioning due to gender identity. According to this study that mentions this, there were 1000-1600 MTF and 400-550 FTM patients, which equates to regret rates of <1% for FTMs and 1-1.5% for MTFs (page 4).
- https://journals.lww.com/prsgo/Fulltext/2021/03000/Regret_after_Gender_affirmation_Surgery__A.22.aspx 2021 systemic review and meta-analysis
What about older studies?
I will be talking about the studies on trans kids, which are the most quoted I have seen. One recent example of quotation is in JK Rowling’s essay:
“I want to be very clear here: I know transition will be a solution for some gender dysphoric people, although I’m also aware through extensive research that studies have consistently shown that between 60-90% of gender dysphoric teens will grow out of their dysphoria.”
But there are a number of flaws with these studies. An analysis of 3 of these studies found this (I’m quoting, and it’s a long quote):
“The 3 largest and most-cited studies have reported on the adolescent or adult gender identities of cohorts who had, in childhood, showed gender “atypical” patterns of behavior. Of those who could be followed up, a minority were transgender: 1 of 44, 9 of 45, and 21 of 54. Most of the remaining children later identified as gay, lesbian, or bisexual (although a small number also was heterosexual).
However, close inspection of these studies suggests that most children in these studies were not transgender to begin with. In 2 studies, a large minority (40 and 25) of the children did not meet the criteria for GID to start with, suggesting they were not transgender (because transgender children would meet the criteria). Further, even those who met the GID diagnostic criteria were rarely transgender. Binary transgender children (the focus of this discussion) insist that they are the “opposite” sex, but most children with GID/GD do not. In fact, the DSM-III-R directly stated that true insistence by a boy that he is a girl occurs “rarely” even in those meeting that criterion, a point others have made. When directly asked what their gender is, more than 90% of children with GID in these clinics reported an answer that aligned with their natal sex, the clearest evidence that most did not see themselves as transgender.
We know less about the identities of the children in the third study, but the recruitment letters specifically requested boys who made “statements of wanting to be a girl” (p. 12), with no mention of insisting they were girls. Barring evidence that the children in these studies were claiming an “opposite” gender identity in childhood, these studies are agnostic about the persistence of an “opposite” gender identity into adulthood. Instead, they show that most children who behave in gender counter-stereotypic ways in childhood are not likely to be transgender adults.”
This analysis of 4 of these studies found methodological, theoretical, ethical, and interpretive concerns. Here is their breakdown:
Methodological Concerns
- the potential misclassification of child research participants
- the lack of acknowledgement of social context for research participants
- the age of participants at follow-up
- the potential misclassification of adolescent and young adult participants lost to follow-up
Theoretical Concerns
- assumptions inherent in“desistance” terminology
- binary gender framework
- presumption of gender stability as a positive outcome
Ethical Concerns
- intensive treatment and testing of child participants
- questionable goals of treatment
- lack of consideration of children’s autonomy
Interpretive Concerns
- the assumption that unknown future adult needs should supersede known childhood needs
- the underestimation of harm when attempting to delay or defer transition
Here are the conclusions from this presentation from a WPATH conference (which is a reputable organization on gender dysphoria), which criticizes some of those studies:
- Evidence from these studies suggests that the majority of gender nonconforming children are not gender dysphoric adolescents or adults.
- It does not support the stereotype that most children who are actually gender dysphoric will “desist” in their gender identities before adolescence.
- These studies do acknowledge that intense anatomic dysphoria in childhood may be associated with persistent gender dysphoria and persistent gender identity through adolescence.
- Speculation that allowing childhood social transition traps cisgender youth in roles that are incongruent with their identities is not supported by evidence.
- These studies fail to examine the diagnostic value of Real Life Experience in congruent gender roles for gender dysphoric children.
I’ll also leave some links that you can look at about those poor studies and this topic in general for further reading (most reference some of the studies I have talked about):
-
https://www.vox.com/2016/8/9/12404246/transgender-children-detransitioning-transphobia
-
https://www.huffpost.com/entry/myths-about-transition-regrets_b_6160626
-
https://rationalwiki.org/wiki/Gender_transition#The_myth_of_high_detransition_rates
-
https://www.huffpost.com/entry/the-end-of-the-desistance_b_8903690
-
https://genderanalysis.net/2015/07/walt-heyer-and-sex-change-regret-gender-analysis-09/
Canada's C-16 Bill
Canada’s C-16 Bill
C-16 is about hate crimes, not pronoun usage. Misgendering doesn’t cross the threshold for being a hate crime in Canada.
- The contents of the bill: “The bill is intended to protect individuals from discrimination within the sphere of federal jurisdiction and from being the targets of hate propaganda, as a consequence of their gender identity or their gender expression. The bill adds “gender identity or expression” to the list of prohibited grounds of discrimination in the Canadian Human Rights Act and the list of characteristics of identifiable groups protected from hate propaganda in the Criminal Code. It also adds that evidence that an offence was motivated by bias, prejudice or hate based on a person’s gender identity or expression constitutes an aggravating circumstance for a court to consider when imposing a criminal sentence.”
- Essentially, hate crimes against people based on gender identity/expression will be treated legally at the same level as other hate crimes, e.g. racially motivated hate crimes
- Not once are pronouns or misgendering explicitly brought up in the bill
- This provides some further clarity on the bill’s purpose: “The recognition of the rights of gays and lesbians has evolved in some measure through the recognition of the right to be free from discrimination based on sexual orientation. Sexual orientation does not necessarily protect those whose gender does not align with their sex assigned at birth, or who do not consider themselves to fit in with conventional conceptions of gender. Bill C-16 seeks in part to add the grounds of gender identity and gender expression to broaden the recognition of the rights of other members of sexual minority groups.”
- Torontoist: Cumming 16
- This article includes a legal expert who comments on C-16 and Jordan Peterson’s takes
- Jordan Peterson, an active critic of C-16, is likely misunderstanding or mischaracterizing the bill
- The threshold for a hate crime in Canada is likely too high for misgendering to be considered a hate crime
- Canadian Broadcasting Corporation 18
- Good brief on what C-16 actually does
- Bill C-16 added the words “gender identity or expression” to three places:
- Canadian Human Rights Act, joining a list of identifiable groups that are protected from discrimination. These groups include age, race, sex, religion, disability, etc.
- A section of the Criminal Code that targets hate speech — defined as advocating genocide and the public incitement of hatred — where it joins other identifiable groups.
- A section of the Criminal Code dealing with sentencing for hate crimes. If there’s evidence that an offence is motivated by bias, prejudice or hate, it can be taken into account by the courts during sentencing.
- Being jailed for repeated misgendering would be very difficult to do even with C-16 in place
Specific Debunks:
- **CLAIM: Father in British Columbia found guilty of ‘family violence’ for misgendering his trans son**
- Case was unrelated to C-16 and had far more to it than misgendering
- The father was actively bringing his trans son’s personal issues to light in public interviews, and brought up personal details during those interviews
- The father was also actively contributing to worsening the child’s mental health (the son had already attempted suicide in part because of his father, for example)
- Legal source in regards to this case, provides more context
- **CLAIM: Anti-gay activist William Whatcott fined $55,000 for misgendering trans activist Morgane Oger**
- Unrelated to C-16, dealt instead with section 7 of British Columbia’s Human Rights Code (keep in mind C-16 was national legislation, not provincial legislation)
- Whatcott was spreading anti-trans misinformation in general, specifically targeting Oger who was running for political office at the time and lost by a small margin
- Original source in regards to this case, provides more context — C-16 not cited in it, aside from the Canadian Human Rights Act being brought up once in 104 pages
In the Military
In the Military
Transgender people should be allowed to serve in the military. There is a notable lack of evidence for transgender personnel disrupting unit cohesion, and other concerns e.g. costs and deployability disruption aren’t THAT big a deal.
- “Assessing the Implications of Allowing Transgender Personnel to Serve Openly” by RAND Corporation, 2016 (full text pdf)
- Study from RAND Corporation about potential impacts of transgender military service. Covers a LOT of ground over the course of NINE chapters, including but not limited to:
- The existing trans military population
- Their healthcare needs
- The impact of letting them serve openly
- DoD policies that would need to be changed to let them serve openly
- ON TRANSGENDER MILITARY ESTIMATES: RAND’s estimates found there are currently 1,320–6,630 active transgender members in the military. This wide range exists in part because of difficulties getting an accurate estimate.
- ON TRANSITION-RELATED HEALTHCARE COSTS: The transition-related healthcare costs would be relatively low for trans people, adding between $2.4m and $8.4m to overall healthcare costs for active service members. That’s a 0.04-0.13% increase in overall costs.
- Some people might think this is a 0.04-0.13% increase relative to the entire military budget. This is not true. This is not for the overall military budget, but rather for costs specifically related to healthcare for active service members.
- It’s important to note that not all of the trans people in the military actively need funds for medical transition. In any given year, RAND found that “Only a subset will seek gender transition–related treatment… between 29 and 129 service members in the active component will seek transition-related care that could disrupt their ability to deploy.”
- ON DEPLOYABILITY IMPACT: Most issues with non-deployability come around during medical transition, mainly in the form of medical leave for having and recovering from transition-related surgeries. This translates to 29-129 people per year getting medical service that could possibly disrupt their ability to be deployed during that mid-transition time period. RAND does recommend additional mental health screening in the specific context of gender dysphoria, at least pre-transition. Those who are post-transition are expected to be safely deployed along the same parameters as other service members (for example, other members also get their mental health screened prior to deployment).
- ON UNIT COHESION IMPACT: Impacts on unit cohesion weren’t found to be a big concern in the report, going off of results from similar integration efforts in the past, e.g. including women and LGB people. They also took a look at other countries (Australia, Canada, Israel, and the UK) that had included trans people in the military, and found no significant impact on unit cohesion in those countries.
- Study from RAND Corporation about potential impacts of transgender military service. Covers a LOT of ground over the course of NINE chapters, including but not limited to:
- Okros & Scott 2014
- Study that analyzed the impact of a transgender-inclusive policy on the operational effectiveness of the Canadian military
- Used FIVE different methods to try and find any negative impacts, e.g. interviews of military experts, people with personal experience, media reports, etc
- Found NO evidence whatsoever that the military’s operational effectiveness suffered from the trans-inclusive policy
- Williams Institute, 2014
- Study that tries to estimate the number of military servicemembers and veterans that are transgender
- Came out with a rather high estimate of 15,500 active servicemembers who are transgender, and around 134,300 transgender people who either are serving or have served in the military before. This translates to around 20% of the transgender population having served in the military at some point.
- For reference, only around 10% of the general population has served in the military at some point, active and veterans included.
- This should emphasize the importance of the discussion around trans people in the military, as so many trans people have gone through it. A ban from the military could have a serious impact on the transgender community.
Brief note on surveys that ask servicemembers how they would feel about a trans military ban: this data isn’t actually useful. Due to the politically charged nature of the topic, responses may not have reflected actual experiences within the military or whatnot, but instead may reflect the political affiliation of respondents. This could make this source useless as a result. This is something I saw in two studies.
- This study set out to survey a diverse group of active duty, cisgender servicemembers and found that overall, 66% supported transgender inclusion into the military. This differed between subsets of the surveyed group. For example, 82% of LGB servicemembers supported transgender service while only 57% of heterosexual ones did. While this study didn’t explicitly ask about political leanings (e.g. right wing, liberal, etc) the results do fall in line a way with how these demographics typically fall politically - LGB people are more liberal and thus more opposed to the ban, heterosexual people tend to be more distributed across both parties and as a result are more split half-and-half in the survey results. This would suggest that certain demographic characteristics correlate with political leanings, which in turn predict people’s stances on these political issues.
- This study surveyed a group of mostly conservative ROTC cadets and Academy cadets and found that a significant portion of them supported a transgender ban in the military. Their typical respondent was “at a military academy, male, white, nineteen or younger, leaning politically to the right, Christian, and in their first (freshman) year of college.” The study also found that “Although cadet attitudes on the surface appear generally negative toward transgender people, the findings have more to do with context, sex, political, and religious beliefs than military culture and affiliation exclusively.” This means that their beliefs about the transgender military ban were better explained by their politics than by their military experience.
If we do want to make a policy decision based on this, though, we could definitely consider improving unit cohesion by decreasing transphobic beliefs in the military, as more transphobic people seem to have more concerns about not being able to work with a trans person.
Trump transgender military ban:
- “DoD’s Rationale for Reinstating the Transgender Ban Is Contradicted by Evidence” by the Palm Center, 2018
- This was specifically written in response to a report published to justify the Trump administration’s transgender military ban**, so it’s specifically responding to the reasoning made for that ban.
- Something worth noting is that this DoD Rationale may have been directed by explicitly right-wing, anti-trans activists like Ryan Anderson, Mike Pence, and Tony Perkins. This makes the DoD’s rationale less reliable as it may have been influenced by agenda-driven actors who are willing to manipulate the evidence to achieve a certain end.
- The DoD report starts out with clearly unreasonable assumptions, mainly that gender transition isn’t particularly effective. Of course, this position goes against nearly all of the existing academic literature and so the DoD report has to cherry-pick 4 studies which still backfires. From the Palm Center critique: “Yet DoD’s findings rely on a selective reading of scholarship. Despite decades of peer-reviewed research, the Implementation Report could identify only four studies to sustain its conclusion. Critically, even these four studies, supposedly representing the best evidence documenting the uncertainty about transition-related care’s efficacy, all conclude that such care mitigates symptoms of gender dysphoria.”
- The Palm Center argues that the transgender ban would create a double standard for transgender people rather than have everyone working along the same medical, fitness, and deployability standards, an approach which weakens the legitimacy of the existing military standards and serves to single out transgender people in a discriminatory way.
- The Palm Center also argues that most trans troops are medically fit, using the DoD’s own data to carry home the point: “Out of 994 service members diagnosed with gender dysphoria in FY2016 and the first half of 2017, 393 (40 percent) deployed in support of Operation Enduring Freedom, Operation Iraqi Freedom, or Operation New Dawn. Exactly one individual deploying with a diagnosis of gender dysphoria was unable to complete the deployment for mental health reasons since policy protecting transgender personnel from arbitrary dismissal was established in June 2016.”
- The transgender ban rationale has certain double standards when it comes to suicide attempts, arguing that the high suicide attempt rate for transgender people should bar them from service while similar high-risk groups oftentimes go ignored, e.g. children of service members (who have a 50% higher suicide attempt rate than the general population). The rationale makes further mistakes with the use of suicidality in its reasoning, and of course fails to account for the fact that stigmatization of trans people (e.g. banning them from the military) has a negative impact on suicidality.
- On the topic of unit cohesion, the DoD Rationale provides no actual real-life evidence that trans inclusion would harm cohesion, instead only providing a handful of hypotheticals. These hypotheticals are dubious in and of themselves and aren’t enough to properly argue that trans people hurt unit cohesion.
- In general, the Rationale fails to consider opposing viewpoints, mainly by failing to address potential downsides of a ban or considering possible missed benefits from inclusion. The Rationale is not a balanced, fair approach at the topic, but a one-sided approach which ends up ignoring valid points which oppose the conclusion they want.
- This was specifically written in response to a report published to justify the Trump administration’s transgender military ban**, so it’s specifically responding to the reasoning made for that ban.
-
APA condemnation of the Trump admin’s transgender military ban
-
AMA condemnation of the Trump admin’s transgender military ban
- Condemnation of the rationale for Trump admin’s transgender military ban by SIX FORMER SURGEONS GENERAL
Depathologization
Depathologization
+ its impact
- https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(15)00022-X/fulltext
- Explains that being trans and/or having gender dysphoria aren’t mental illnesses in themselves, and that mischaracterizing these as a mental illness is wrong in a number of ways:
- Properly reflect what it means to be transgender and rightfully shift the troubles specific to gender dysphoria towards gender dysphoria rather than transness as a whole
- Better guide medical researchers, policymakers, and the public regarding proper understanding of what it means to be transgender and how to apporach those issues
- Reduce the potential for unjustified stigmatization/discrimination of trans people
- Explains that being trans and/or having gender dysphoria aren’t mental illnesses in themselves, and that mischaracterizing these as a mental illness is wrong in a number of ways:
-
https://www.scientificamerican.com/article/where-transgender-is-no-longer-a-diagnosis/
-
https://icd.who.int/browse11/l-m/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f411470068
- https://pubmed.ncbi.nlm.nih.gov/27492343/
-
https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366%2816%2930165-1/fulltext
-
https://academic.oup.com/fampra/article-abstract/38/4/543/6300602 maybe just not have this source
-
https://www.euro.who.int/en/health-topics/health-determinants/gender/gender-definitions/whoeurope-brief-transgender-health-in-the-context-of-icd-11 this one looks useful, circle back to that one
- http://www.cakeworld.info/transsexualism/illness
- Blog post that takes a broader stance of “whether or not it’s a mental illness to be trans (a matter largely of semantics), that doesn’t change the fact that gender dysphoria can be mentally debilitating and we should allow people to get medical treatment for gender dysphoria”.
- Also acknowledges that characterizing trans people as inherently having a mental illness opens the door to sigmatization and discrimination
- https://www.apa.org/topics/lgbtq/transgender “A psychological state is considered a mental disorder only if it causes significant distress or disability. Many transgender people do not experience their gender as distressing or disabling, which implies that identifying as transgender does not constitute a mental disorder.”
Addressing Reactionary Claims
Addressing Reactionary Claims
Some claims about trans people are addressed in this doc by this person, if you want to take a look. This webpage, this document and this second webpage also have a lot of material to work with. Certain myths have also been addressed elsewhere in the Source Library on this page.
WIP section but will probably cover:
-
Mia Forstater and JK Rowling controversies
-
The claim that trans people reinforce gender stereotypes
Q: What about the failed David Reimer case study, which was led by John Money, who introduced the gender-sex distinction? Doesn’t this failure not only suggest that his gender-sex distinction is flawed, gender roles are tied to nature rather than nurture, and that trans people by extension can’t change their nature via transition?
-
It’s highly encouraged that you read about the experiment and Reimer’s life before trying to refute claims made about them. His wikipedia page is a good start, but there are a number of other biographies and articles about him which could be worth reading through as well.
-
The David Reimer case is tragic and Money should never have experimented with Reimer in the ways he did. Money covered up the negative results of the experiment for years. There is no reason to defend the ethicality of this whatsoever.
- This does not properly represent the situation with trans people today, however. Reimer was forced into a girl’s gender roles at a young age and was given hormones basically at birth, unlike cases nowadays where trans people actively want to transition rather than being forced into such. Reimer’s case applies best to people who are forced into transitioning despite not wanting it.
- If anything, the Reimer case undermines anti-trans activists insofar that it shows the harmful impacts of being forced to live under a gender identity you didn’t choose for yourself. In this case, we see Reimer, a cis man, suffer from being forced into a trans identity against his will. This exact same situation could apply to a trans person being forced into a cis identity against their will - you just swap “cis” and “trans” with each other.
- The comparison of Reimer to trans people today is further strengthened in that Reimer basically had gender dysphoria as a woman, which is described in depth in his long-term follow-up with Milton Diamond in 1997:
- “There were little things from early on. I began to see how different I felt and was, from what I was supposed to be. But I didn’t know what it meant. I thought I was a freak or something; … I looked at myself and said I don’t like this type of clothing, I don’t like the types of toys I was always being given, I like hanging around with the guys and climbing trees and stuff like that and girls don’t like any of that stuff. I looked in the mirror and sees my shoulders are so wide, I mean there is nothing feminine about me. I’m skinny, but other than that, nothing. But that is how I figured it out. [I figured I was a guy] but I didn’t want to admit it, I figured I didn’t want to wind up opening a can of worms.”
- “Joan was put on an estrogen regimen from the age of 12 years but rebelled against taking the hormones. They made her “feel funny” and she didn’t want to feminize. She would often dispose of her daily dose. She unhappily developed breasts but wouldn’t wear a bra. Things came to a head at the age of 14. In discussing her breast development with her endocrinologist she confessed “I suspected I was a boy since the second grade”.
- This specific case doesn’t really disprove anything about the gender-sex distinction, and the distinction has been validated by further research showing that your biological sex and gender identity don’t always align normally. This experiment is far better for proving the existence of gender being rooted mostly in nature, a statement which might not even conflict with the concept of trans people (assuming their transgender identity also has neurological/biological basis). In fact, the primary focus of Money’s experiment was on the nature-nurture question, not on if a gender-sex distinction was useful. Just because Money, a bad person, introduced the distinction, that does not automatically make the distinction useless or bad.
- The gender-sex distinction is actually helpful for analyzing the Reimer experiment. Here, we see that he has a male biological sex, yet is forced into the gender identity of a woman. The sex-gender distinction is pretty clearly in play with this analysis, proving itself to be useful.
Q: Why didn’t the medical community change courses on anything or drop any bad ideas after the Reimer experiment went wrong? Doesn’t that indicate corruption and a leftist agenda?
-
Part of why the medical community didn’t change in response to the bad results sooner is because those bad results were covered up by Money for years. John Money boasted that his experiment had been a success and the medical community accepted what he said as true for years, until David Reimer collaborated with Dr. Milton Diamond and, in 1997, published a long-term follow-up for Money’s earlier experiments which rebutted Money’s research and got worldwide attention. Only then was the truth about Money’s experiment actually available to the medical community for them to actually make changes in response to.
-
Once the medical community was aware of the truth, changes were made though. This case, which was mainly focused on the nature-nurture question and gender plasticity, opened up that discussion while severely undermining the “it’s mostly nurture” side of the aisle. It also led to medical reforms on the issue of sex reassignment surgery for infants with certain defects (e.g. micropenis). You can read more about that specifically here, in the Social Impact section.
Q: What if I identify as an attack helicopter, or as a different age? Should I be given the same respect in my identity as trans people want for themselves?
-
This is a false analogy on its face, helicopters and different ages are not analogous to gender identity; helicopters aren’t even socially constructed (while gender is) and age, while being a social construct (humans constructed the measurement of time via years, months, etc), is not tied to the certain behaviors or identification of a person like gender is.
-
The comparison made implicitly assumes that men and women are about as different as humans are to helicopters, which is clearly a bad analogy to use here. As it turns out, men and women are both human and share a lot beyond that while helicopters aren’t even sentient.
-
This started out as a dumb joke, and isn’t well-equipped at all to be an actual argument. Anyone who uses this as a legitimate argument has no idea what they’re talking about.
-
This page gives a different approach to the attack helicopter arg
(WORK IN PROGRESS) Q: What if I identify as an attack helicopter, or as a different age? Should I be given the same respect in my identity as trans people want for themselves?
- There’s a couple things implied with this argument, which we’ll refute here.
- Certain things don’t fit within the parameters of gender identity/expression (e.g. identifying as an attack helicopter because attack helicopter is a gender or the sort). Gender expression deals specifically with how a person chooses to express themselves within society as a human being. Gender does NOT deal with whether people are human, dogs, attack helicopters, etc.
- People already recognize this insofar as they know being a human, dog, cat, etc. is different from being a boy or a girl. Masculine dogs exist alongside feminine dogs, and these dogs are able to present themselves as masculine and feminine while still being dogs. Heck, sometimes people even apply gender identificative terms to inanimate things, e.g. countries (“Mother Russia” or the “Fatherland” for Germany) and referring to war ships in a feminine way (which is a traditional thing to do, not a new SJW thing).
- Some people will argue “if I can identify or express myself as a woman, why can’t I express myself as being a different age or height or whatever?” These people don’t know that the parameters of gender identity/expression don’t necessarily apply to other things (e.g. age or height).
- Certain things don’t fit within the parameters of gender identity/expression (e.g. identifying as an attack helicopter because attack helicopter is a gender or the sort). Gender expression deals specifically with how a person chooses to express themselves within society as a human being. Gender does NOT deal with whether people are human, dogs, attack helicopters, etc.
Q: What about Ray Blanchard’s theory of autogynephilia, the idea that most or all trans women are trans because of erotic arousal by the thought of being a woman?
-
Most evidence supporting the theory was published by Blanchard himself prior to 2003, after which his theory and methodology were both criticized
-
https://juliaserano.blogspot.com/2015/07/the-real-autogynephilia-deniers.html nice roundup of the research surrounding autogynephilia
- A few direct critiques of the theory and/or methodology:
-
https://www.researchgate.net/publication/26660017_Autogynephilia_in_Women the behaviours characterized as autogynephilia was observed on a frequent basis in 28% of women
-
https://juliaserano.medium.com/making-sense-of-autogynephilia-debates-73d9051e88d3 more julia serano content
-
https://www.reddit.com/r/musicotic/comments/9n3zsu/autogynephilia_myths_version_20/
- https://sillyolyou.wordpress.com/tag/autogynephilia/
Q: People with anorexia are treated with psychiatric help, not hormones or surgery. Why can’t we do the same for trans people?
- There’s a crucial set of differences between people with anorexia and those with gender dysphoria.
- People with anorexia are wrong from the outset when they assume they are overweight, when they’re not. When a person with gender dysphoria thinks they don’t pass as their desired gender, they’re usually not wrong at all, especially if they haven’t gone through any sort of transition to their desired gender yet.
- Anorexic people usually respond well to psychiatric treatment, whereas the similar curative/conversion therapy option for trans people has yet to emerge as a successful treatment. As for affirmation, trans people respond well to affirmation (See: Medical Transition section of this page) whereas affirming anorexic people’s beliefs don’t lead to good results (and any good results from starving an underweight person are probably outweighed by convincing them they’re not overweight to begin with).
-
Some people cite body dysmorphic disorder or body dysmorphia instead of anorexia specifically. The same basic framework applies between anorexia and BDD.
-
While gender dysphoria and BDD/anorexia are not really comparable in the way of treatments, it’s important to note that they can happen in relation to each other. For example, someone who is very conscious about their body image due to dysphoria might develop BDD as a result of that anxiety. However, that doesn’t justify approaching both gender dysphoria and BDD with the same treatments.
- This talking point is addressed here as well
Q: Don’t you need dysphoria to be trans?
Similar to the gender-sex distinction, the answer to this question largely comes down to semantics. It also comes down to whether or not some trans people have managed to get rid of their dysphoria. Let’s start with the semantic aspect. Below are a number of medical organizations cited where they implicitly or explicitly say that not all transgender people have to deal with gender dysphoria:
| Organization | Quote |
|---|---|
| American Psychiatric Association | Not all transgender people suffer from gender dysphoria and that distinction is important to keep in mind. Gender dysphoria and/or coming out as transgender can occur at any age. |
| World Health Organization’s ICD-10 | A desire to live and be accepted as a member of the opposite sex, usually accompanied by a sense of discomfort with, or inappropriateness of, one’s anatomic sex, and a wish to have surgery and hormonal treatment to make one’s body as congruent as possible with one’s preferred sex. |
| American Psychological Organization | Many transgender people do not experience their gender as distressing or disabling |
| American Academy of Pediatrics | Some youths experience gender dysphoria when the incongruence between assigned sex at birth |
| Canadian Paediatric Society | Some transgender children experience no distress about their bodies, while others may express significant discomfort. |
| World Medical Association | The WMA asserts that gender incongruence is not in itself a mental disorder; however it can lead to discomfort or distress, which is referred to as gender dysphoria (DSM-5). |
| World Professional Association for Transgender Health | The various The DSM-5 descriptive criteria for gender dysphoria were developed to aid in diagnosis and treatment to alleviate the clinically significant distress and impairment that is frequently, though not universally, associated with transsexual and transgender conditions. |
If that’s not convincing, let’s go on to that second part: if you have a transgender person who used to have dysphoria, but has now gone through so-and-so procedures and now feels in line with their body, no longer feels dysphoric… is that person no longer transgender? Obviously not. So that again goes to show that you can be transgender without necessarily having dysphoria.
Q: Doesn’t transition sterilize trans people?
Not always. It depends on the aspects of transition someone chooses to go through - for example, an FTM trans man who goes through HRT will not go sterile, but he will go sterile if he goes through a hysterectomy (surgical removal of the womb). In fact, there is documented evidence of trans men going through pregnancy (this means they’re not sterile), a majority of whom had been on testosterone. It’s worth noting that some countries do not offer legal recognition to trans people unless they are sterilized, which is discriminatory and against human rights law.
Specific Studies and Articles:
- Dhejne et al. 11 (sometimes referred to as the Sweden study), study name “Long-Term Follow-Up of Transsexual Persons Undergoing Sex Reassignment Surgery: Cohort Study in Sweden”
- Commonly cited by anti-trans activists to indicate sexual reassignment surgery harms trans people, increases risk of suicide.
- This is NOT what the study says
- A study proving that SRS harms trans people would compare the wellbeing of post-SRS trans people to pre-SRS trans people, but this one uses CIS people as a control group. Because of this, we can only use the data to compare certain trans people to the cis population - we can’t compare pre-SRS to post-SRS with this data.
- An excerpt from the study - “no inferences can be drawn as to the effectiveness of sex reassignment as a treatment for transsexualism. In other words, the results should not be interpreted such as sex reassignment per se increases morbidity and mortality. Things might have been even worse without sex reassignment.”
- The study merely demonstrates that trans people who have had SRS still are a vulnerable population compared to cis people, but NOT that their condition had been worsened by SRS.
- The head author, Cecilia Dhejne, is actually very trans positive herself, and describes her intent in publishing this study in this Reddit AMA. She also clarifies what the study says in this interview.
- From the Reddit AMA: “I have said many times that the study is not design to evaluate the outcome of medical transition. It DOES NOT say that medical transition causes people to commit suicide.”
- From a different published work by Dhejne directly summarizing the study: “This study cannot determine the effectiveness of gender-affirming medical intervention”
- On top of all of this, a different study also focused on Sweden reaffirmed that SRS leads to satisfaction in the long run (though this one had 5 years of data while the Dhejne study had 20 years). A different study, also conducted in Sweden and with Dhejne as the lead author, found that the regret rate for transitioning was a measly 2.2%
- Something important to note about the time period of this study is that societal attitudes toward transgender people may have changed during the study’s timeframe, between 1973 and 2003. The same is true for transgender healthcare itself. This means that the outcomes of transitioning in 1970 could very well differ from the outcomes of transition in 1990.
- “In accordance, the overall mortality rate was only significantly increased for the group operated before 1989. However, the latter might also be explained by improved health care for transsexual persons during 1990s, along with altered societal attitudes towards persons with different gender expressions.”
- Brief on the study’s misuse in this video https://youtu.be/WNjdTNYzWbc?t=1037 17 minutes in
- This study is also cited to prove that “trans women retain male pattern violence” and was misrepresented so much that the author herself had an interview to discuss how that’s not what the study is saying. This article by Gemma Stone goes over this specific talking point.
- Littman 18 (more info here, very thorough rebuttal here)
- Just to note at the start, this study has gone through debunk after debunk after debunk after debunk after debunk after debunk. There’s so many ways in which this study is wrong and so many rebuttals of the study that rebutting it has become a dead horse at this point.
- Commonly cited by anti-trans activists to indicate transness spreads socially, that exposure to trans material might encourage youth to be trans. “Rapid Onset Gender Dysphoria” (ROGD).
- The polls were taken on sites which were biased by nature - ‘4thwavenow, transgendertrend, youthtranscriticalprofessionals’. Parents who frequent these sites will have already been conditioned to doubt their kids’ trans identity, so will be much more likely to subscribe to ROGD as a justification for their beliefs. This is already reason enough to dismiss the study as a proof of ROGD - it’s hard to get any reliable conclusions out of bad data.
- On top of this, the study specifically targeted parents who would fit the ROGD hypothesis, reaching out to “parents of teens who became convinced they were the opposite sex after a steady diet of social media and/or peer influence”. This sample was probably recruited with intent to prove that ROGD is a big thing, or at the very least to prove that gender dysphoria is a social contagion.
- It also doesn’t help that the idea for ROGD first surfaced via these specific websites (though Littman popularized the term “Rapid Onset Gender Dysphoria”) and not from previous scientific inquiry (Littman’s study was the first one ever on ROGD!), which further suggests that these specific websites were hand-picked by Littman to prove a specific hypothesis.
- Furthermore, the study polled parents instead of children, which makes the data even less reliable. While polling parents isn’t always a bad thing, it really undermines this particular study for a number of reasons:
- Parent evaluations vs children self-evaluations tend to differ substantially when it comes to mental health, and is even more an issue when the parents are stressed about it (as detailed here in the 4th paragraph). Parents of trans kids who frequent websites about a “transgender craze” going down are probably going to be stressed because they’ll think their kid is involved in this craze.
- What appears to a parent to be a “rapid” onset may not have been rapid for their child at all, as closeted LGBTQ children tend to stay closeted for a while before coming out (they still fear discrimination/rejection by their family, among other things) and during this time they’ll get a better sense of their gender identity or sexual orientation. When a gay or trans person comes out of the closet to their parents, what the kids had to process over the course of months or years is processed by parents over the course of mere days - so what looks like a rapid change to parents could easily be anything but rapid to trans children.
- Even if we are dealing with something which is genuinely rapid-onset, not just from the parent’s view but also from the child’s, this isn’t necessarily a bad thing. To quote from Julia Serano: “There is nothing inherently erroneous or illegitimate about a “rapid” onset of gender dysphoria — some trans people experience an epiphany during which all the clues and puzzle pieces suddenly come together, and they finally realize that they are transgender.” This just goes further to show that the element of social contagion still might not be supported by this study, even if we assume the data is 100% accurate.
- Multiple other important critiques are made here if you want a look, this gives a lot more insight into how Littman’s study is flawed (including criticism of the DSM-5 model used).
- “But, the study got censored and suppressed by the activist left! Even disregarding flaws, doesn’t that suggest a biased academia?”
- The study was never even pulled from the journal it was published in, despite its many flaws; it’s still there and available in full. That’s not suppression and that’s not censorship.
- As for the Brown University press release on the study, it was retracted not due to a political agenda but because of concerns raised about the study quality and design - which definitely exist for this study. Suppressing a press release (not the actual study) on a badly designed, fatally flawed study is not a bad thing to do. See the “Expanded Brown University Statement – Tuesday, Sept. 5, 2018” linked here.
- Regardless, there’s been a good amount of debate on the merits of Littman’s study. A good example of this in play would be from this back-and-forth about the study. Keep in mind that criticizing a study isn’t the same as trying to censor it.
- “But, the study also found that kids going through ROGD also consumed a lot of trans media and/or had trans friends! Doesn’t that suggest social contagion?”
- You could just as easily suggest that the situation is actually flipped - it makes sense for a closeted person with gender dysphoria to seek out other people with gender dysphoria, rather than vice versa. Marginalized groups of people tend to seek out one another to get advice or feel comforted by someone whose experiences they can relate to. This applies to a trans person who is closeted (in which case the parents wouldn’t know their kid was trans until the kid comes out as trans). In fact, it’s well documented that gay people reach out to gay communities for help going out of the closet, as it is for people of various political ideologies when they deal with coming out to their loved ones (most commonly a conservative coming out to their liberal family or vice versa). This same sort of process happens with trans people and trans communities.
- Leinung et al. 18 sometimes cited as this article
- The study claims that hormonal therapy does not help reduce testosterone levels to that of a cis woman’s
- However, the study uses the testosterone blocker known as Spiro, which inhibits testosterone receptors rather than stopping its production, making the data useless. On the other hand, a different study (non-paywall) using Cypro (a testosterone blocker that actually lowers testosterone in the blood) shows testosterone levels lower than average female levels. This doesn’t mean that HRT doesn’t reduce testosterone, but only that a certain form of HRT isn’t that effective.

- PBS: Women fear drug they used to halt puberty led to health problems
- Commonly cited by anti-trans activists in order to try and prove the false claim that puberty blockers are harmful
- The girl in the article had precocious puberty (puberty starting too early), which can be dangerous if untreated
- The effects cited are common from using the medication for too long and or using the wrong dose, meaning its the fault of the doctor and not the medication
- The article does not prove puberty blockers are bad, it proves doctors need to do better
- A Wiik et al. 2019: Muscle strength, size and composition following 12 months of gender-affirming treatment in transgender individuals: retained advantage for the transwomen
- The study is not peer reviewed despite how long its been up
- Bad methodology: the study doesn’t take into account outside influence on muscle mass such as manual labor or exercise neither pre hrt nor during the treatment, which can provide a big starting point regardless of sex hormones, Something which compares trans athletes and trans people who aren’t as active would provide more accurate data
- The Federalist: “Study: Transgender Male Athletes Keep Physical Advantages Even After Female Hormone Injections”
- Big conservative bias with a conspiracy theory and very incorrect use of words in the first paragraph
- The study did not talk about trans women at all, it talked only about suppressing testosterone without introducing cross sex hormones
- This study is taken completely out of context and doesn’t prove anything about trans women.
- The rest of the article draws conclusions from that ONE study that doesn’t even prove the point they try to make and makes it seem like that’s all science has to offer.
- Dirks 18 (pdf)
- Cited by anti-trans activists to indicate that gender inclusion policies in store changing rooms leads to a large increase in sexual offences
- BAD DATA COLLECTION: The study uses media reports from Google searches, which is a horrific way to collect data on actual sexual offences.
- If a single incident gets reported on by multiple outlets, that may have been counted as multiple incidents by the study.
- The amount of reporting on these incidents in Target stores may have had an uptick after the policy was passed as more people were interested in those particular sorts of incidents.
- Most cases recorded in the database did not even take place in the changing rooms or bathrooms, which is what the gender non discriminatory policy affected, but rather the store floor (using ctrl + f, there were 17 mentions of ‘washroom,’ 50 mentions of ‘changeroom,’ and 155 mentions of ‘store’ (as in store floor) on the database).
- Despite the vast majority of upskirt incidents happening on the store floor (97.1%), with, again, store floors not being affected by the policy, and the vast majority of peeping tom incidents happening in changing rooms and bathrooms (98.4%), both went up by almost the exact same rate: ‘In a Poisson regression, using trimesters to control for seasonal variations in offenses,the fold change in rate from the four year pre-policy period to the post-policy period was 3.03 for Upskirt and 3.14 for Peeping Tom.’ This means the policy can explain almost none of the rise in these cases, but rather most likely the methodology (as it relies only on media reports). And these numbers are from the study itself!
- It is not peer reviewed and published on Woman Means Something, a TERF website.
- The study’s author is a pastor who supports gay conversion therapy, showing further study bias - people who are anti LGB are very likely to also have conservations about the T
- Anyway, there is a large consensus of US sexual assault charities that have come forward in support of trans-inclusive policies
- Those 4 studies that show ~80% detransition in children
-
http://www.thenewatlantis.com/docLib/20160819_TNA50SexualityandGender.pdf (and paul mchugh more broadly)
- Do trans- kids stay trans- when they grow up? from sexologytoday.org by James Cantor
- Most of these studies are grossly out of date, with only 4/11 of them being from after 1990. That means that most of the studies cited are over 30 years old! Studies this old also tend to suffer from a host of methodological problems addressed in the Detransition/Regret section of the Source Library.
- In general, the post grossly misrepresents the content of the studies and what each of them found. Rather than cover each and every study here though, it’s much easier to link this video from Jangles Sciencelad which addresses the blog post at around 9 minutes in.
- Another rebuttal on Reddit which also takes some stuff from the Source Library itself
- Hilton & Lundberg 20, study name “Transgender Women in the Female Category of Sport: Perspectives on Testosterone Suppression and Performance Advantage”
- Jangles ScienceLad rebuttal: https://www.youtube.com/watch?v=6VtjgZF9RE8
- Brief deep dive: https://threadreaderapp.com/thread/1494081618348507140.html
- Paul Mchugh WSJ op-ed: “Transgender Surgery Isn’t the Solution”
- 2004 Guardian piece “Sex changes are not effective, say researchers”
- Worth noting, of course, that this was published in 2004. Since then, a renewed mainstream and academic interest in trans issues has led to a mountain of new research since then
- The original ARIF study the Guardian article talked about DID NOT CONCLUDE that sex changes are ineffective, but rather concluded that there were no high quality studies on the subject. That’s furthered discussed here: http://www.cakeworld.info/news/2014-08-02acommentaryonthe2004arifstudyandtheguardianarticlesexchangesarenoteffectivesayresearchers
- Anything which cites Dr David Bell such as the following articles
- ■ David Bell: Tavistock gender clinic whistleblower faces the sack
- ■ Children have been very seriously damaged’ by NHS gender clinic, says former Tavistock staff governor
- ■ Transgender children who are medically treated risk ‘serious and irreversible damage’, leading psychiatrist warns
- Dr David Bell never worked for GIDS. As told by a freedom of information request “Dr Bell has now retired from the Trust. Dr Bell did not work in our GIDS service.” The request can be found here
- BBC: “We’re being pressured into sex by some trans women’”
- Abigail Shrier’s book “Irreversible Damage”
- Heritage Foundation’s “Puberty Blockers, Cross-Sex Hormones, and Youth Suicide” report
- This Heritage report claims that gender-affirming healthcare leads to more suicides among trans youth.
- HORRIBLE METHODOLOGY. This is broken down in the next few bullet points.
- The author tries to measure how accessible gender-affirming healthcare is for trans youth, but instead of looking at laws or clinical policies, he decided to use Google Trends search terms as a proxy of information. He chose vague search terms like “transgender” and “gender dysphoria” which doesn’t really gauge how accessible trans healthcare is, however it does gauge the public’s interest in trans people. These are two very different things which are not simply interchangeable.
- The author also tries to make conclusions about trans youth suicides, but he never actually uses data specific to trans people. Instead, he pulls general suicide data for all of Gen Z and decides that somehow this reflects the specific situation for trans youth. His report doesn’t include any data whatsoever that’s specific to trans youth, even though this is the group of people he’s making such sweeping conclusions about.
- The author notices that as transgender-related search terms increased, so did the suicide rate among Gen Z. However, this doesn’t mean that the transgender debate or trans people is the big thing fueling Gen Z’s depression. Correlation doesn’t automatically mean causation. In fact, there’s a number of other factors influencing Gen Z’s higher levels of suicidality and those factors are well documented - chalking it all up to “more trans healthcare” is insane.
Additional Resources
Additional Resources
- ASAP Science: “The Science of Being Transgender”
- A more concrete, scientific approach towards how we view the causes and meaning of gender identity.
- American Psychological Association
- American Psychological Association pamphlet on transgender issues
- Affirms psychological consensus - that transgender people are valid, have existed throughout history, are subject to discrimination, and that transness is not a mental disorder.
- More food by APA
- American Psychological Association 08
- Gender Identity Resolution which expands upon the premises listed in the annotation above and supports total equality for transgender people - affirmation of the institutional legitimacy of transness in psychology.
- American Psychological Association 14
- Identical to the above, essentially, except pertaining to trans and gender-nonconforming youth.
- American Psychological Association Policy
- Booklet on LGBTQ issues from the American Psychological Association, outlining their policy and attitudes towards aforementioned communities.
-
Expressly positive.
- NHS
- The UK’s National Health Service report on gender dysphoria, which affirms the validity of trans people and discusses ways in which gender dysphoria can be alleviated, the best of which is said to often be social and physical transition.
- American Psychoanalytic Association 12
- The American Psychoanalytic Association’s statement on gender identity, in which transness is validated, social stigma against transgender people is cited as a serious cause of harm and ‘reparative therapy’ - attempts to suppress one’s transness and force them to live as the gender they were assigned at birth - is medically invalid.
- Time: Haynes 19
- The World Health Organization recently stopped classifying transness as a mental disorder.
- United Nations
- Transphobia is cringe, according to the UN
- TGEU 18
- 16 countries in Europe & Central Asia still require sterilization before transgender peoples’ gender identity can be legally recognized
- United nations human rights: Practices of so-called “conversion therapy”
- “Other techniques include trying to make patients’ behaviour more stereotypically feminine or masculine or teaching heterosexual dating skills. Practices aimed at changing gender identity include preventing trans young people from transitioning”
- https://docs.google.com/document/d/1cEPWbmsN9fr0pnwxjls7EVxgZpSGlVOoVqevf2Wcip4/edit
- A few rebuttals to some common anti-trans articles (they pull a lot of arguments from source library btw)
-
https://www.glaad.org/files/aa/2017_GLAAD_Accelerating_Acceptance.pdf
-
https://www.suicideinfo.ca/resource/transgender-people-suicide/
-
https://www.sciencenewsforstudents.org/article/gender-when-body-and-brain-disagree
- Stotzer et al 2014
- 2014 review of research regarding transgender parenting - 51 papers analyzed
- More research is needed (of course) to get a fuller understanding of those situations, but some broad themes regarding discrimination, parent-child relations, etc have emerged
- Discrimination/transphobia is still major issue, e.g. in child custody cases, adoptions, and so on
- Coming out as trans can have a big impact on the parent’s relationship with other family members, with a variety of possible results. Sometimes relationships improve after coming out, sometimes they get worse.
- Some transgender parents said they would benefit from services tailored to their specific needs, e.g. trans parent support groups.
- Interesting read, but the research on this specific topic is young so there’s a lot that’s just not conclusive. Also worth noting more research has come out since 2014 which this paper doesn’t account for
- https://genderanalysis.net/